Pobierz prezentację
1
Cele leczenia hipolipemizującego. Jak je osiągnąć ?!

2
Different stages of atherosclerotic plaque development
Historia naturalna miażdżycy Different stages of atherosclerotic plaque development Figure 8 There are six stages of development of AS: Grades I – IV: accumulation of lipids, first intracellularly, then extracellularly; Grade V: fibrosis around the lipid core forming an atherosclerotic plaque; Grade VI: complicated plaque (rupture, clot or bleed) leading to a clinical event. Fruchart J.C. Handbook of Dyslipidemia and Atherosclerosis
 leading to a clinical event. Fruchart J.C. Handbook of Dyslipidemia and Atherosclerosis.")
3
Kliniczne manifestacje miażdżycy
Ośrodkowy układ nerwowy Udar niedokrwienny Przemijający napad niedokrwienia Serce Zawał serca Dławica piersiowa (stabilna, niestabilna) Tętnice kończyn dolnych Krytyczne niedokrwienie, chromanie przestankowe Vascular disease is the result of a generalized process that may affect any of several vascular beds involving the cerebral, coronary, and peripheral arteries1. Cerebrovascular disease in cerebral arteries may precipitate a transient ischemic attack (TIA) or an ischemic stroke. A TIA, by definition, lasts for fewer than 24 hours. The majority clear within 1 hour. A TIA may be a warning of an impending stroke, with the risk for a stroke being 4% to 8% during the first month following a TIA and 24% to 29% during the next 5 years.1 Coronary vascular disease produces a spectrum of ischemic coronary syndromes that include stable angina, unstable angina, non–ST-segment elevation myocardial infarction (NSTEMI; also known as non–Q-wave MI), and ST-segment elevation (STEMI; also known as Q-wave MI).2 Peripheral arterial disease (PAD) produces a variety of symptoms ranging from intermittent claudication to pain at rest.3 Patients with the most serious form of PAD develop a critical limb ischemia that produces pain at rest and threatens the viability of the limb by increasing the risk for gangrene and necrosis.3 PAD is a strong marker for cardiovascular disease. References 1 Feinberg WM, Albers GW, Barnett HJ, et al. Guidelines for the management of transient ischemic attacks. Circulation. 1994;89: 2 American Heart Association. Heart Disease and Stroke Statistics–2003 Update. Available at: 3 Weitz JI, Byrne J, Clagett GP, et al. Diagnosis and treatment of chronic arterial insufficiency of the lower extremities: a critical review. Circulation. 1996;94:
 Tętnice kończyn dolnych. Krytyczne niedokrwienie, chromanie przestankowe. Vascular disease is the result of a generalized process that may affect any of several vascular beds involving the cerebral, coronary, and peripheral arteries1. Cerebrovascular disease in cerebral arteries may precipitate a transient ischemic attack (TIA) or an ischemic stroke. A TIA, by definition, lasts for fewer than 24 hours. The majority clear within 1 hour. A TIA may be a warning of an impending stroke, with the risk for a stroke being 4% to 8% during the first month following a TIA and 24% to 29% during the next 5 years.1. Coronary vascular disease produces a spectrum of ischemic coronary syndromes that include stable angina, unstable angina, non–ST-segment elevation myocardial infarction (NSTEMI; also known as non–Q-wave MI), and ST-segment elevation (STEMI; also known as Q-wave MI).2. Peripheral arterial disease (PAD) produces a variety of symptoms ranging from intermittent claudication to pain at rest.3 Patients with the most serious form of PAD develop a critical limb ischemia that produces pain at rest and threatens the viability of the limb by increasing the risk for gangrene and necrosis.3 PAD is a strong marker for cardiovascular disease. References. 1 Feinberg WM, Albers GW, Barnett HJ, et al. Guidelines for the management of transient ischemic attacks. Circulation. 1994;89: American Heart Association. Heart Disease and Stroke Statistics–2003 Update. Available at: identifier= Weitz JI, Byrne J, Clagett GP, et al. Diagnosis and treatment of chronic arterial insufficiency of the lower extremities: a critical review. Circulation. 1996;94:")
4
Klasyfikacja dyslipidemii wg Fredricksona (WHO)
Fenotyp I IIa IIb III IV V Podwyższone lipoproteiny Chylomikrony LDL LDL i VLDL IDL VLDL i chylomikrony Aterogenność - +++ + Występowanie Rzadkie Częste Pośrednie Cholesterol w surowicy norma lub TG norma The Fredrickson classification was the first classification of dyslipidaemias. It was based on the analysis of plasma for various lipoprotein fractions, but took no account of the underlying aetiology of any of the dyslipidaemias. In addition, high-density lipoprotein (HDL) cholesterol levels are not considered in this classification.1 Today it is more common to identify the dyslipidaemias by the particular lipoprotein or apolipoprotein that is abnormal. Once dyslipidaemia has been identified it is important to determine the cause where possible. Dyslipidaemia may be secondary to other disorders or a primary abnormality. Common causes of secondary dyslipidaemia include: diabetes mellitus, the nephrotic syndrome, chronic renal failure, hepatobiliary disease (generally of the obstructive variety) and hypothyroidism. It should be recognized that these cause some but not all dyslipidaemias. For example, diabetes can lead to elevation of triglyceride-rich lipoproteins and reduction of HDL, but does not necessarily increase the levels of LDL. On the other hand, hepatobiliary disease is associated with an increase in the levels of LDL. Of the primary causes of dyslipidaemia, the most severe forms are caused by genetic disorders of lipoprotein metabolism. The most easily identifiable in clinical practice are familial hypercholesterolaemia (FH), polygenic hypercholesterolaemia and familial combined hypercholesterolaemia, all of which increase the risk of premature development of CHD. FH is an autosomal dominant disease with defects in the gene for the LDL receptor. Patients presenting with severe forms of hypercholesterolaemia should undergo family screening to detect other family members for therapy.2 Therapy of these disorders is directed towards aggressive management of hypercholesterolaemia with a goal LDL-C that depends on the overall coronary risk of the affected person.2 References 1. Yeshurun D, Gotto AM. Southern Med J 1995;88(4):379–391. 2. Expert Panel on Detection, Evaluation, and Treatment of High Blood Cholesterol in Adults. JAMA 2001:285;2486–2497. Adapted from Southern Med J 1995;88:379–391, with permission from Lippincott Williams & Wilkins. LDL – lipoproteiny o małej gęstości; IDL – lipoproteiny o pośredniej gęstości; VLDL – lipoproteiny o bardzo małej gęstości. (lipoproteiny o dużej gęstości(HDL) nię są uwzględnione w klasyfikacji Fredricksona) Yeshurun D, Gotto AM. Southern Med J 1995;88(4):379–391
 cholesterol levels are not considered in this classification.1 Today it is more common to identify the dyslipidaemias by the particular lipoprotein or apolipoprotein that is abnormal. Once dyslipidaemia has been identified it is important to determine the cause where possible. Dyslipidaemia may be secondary to other disorders or a primary abnormality. Common causes of secondary dyslipidaemia include: diabetes mellitus, the nephrotic syndrome, chronic renal failure, hepatobiliary disease (generally of the obstructive variety) and hypothyroidism. It should be recognized that these cause some but not all dyslipidaemias. For example, diabetes can lead to elevation of triglyceride-rich lipoproteins and reduction of HDL, but does not necessarily increase the levels of LDL. On the other hand, hepatobiliary disease is associated with an increase in the levels of LDL. Of the primary causes of dyslipidaemia, the most severe forms are caused by genetic disorders of lipoprotein metabolism. The most easily identifiable in clinical practice are familial hypercholesterolaemia (FH), polygenic hypercholesterolaemia and familial combined hypercholesterolaemia, all of which increase the risk of premature development of CHD. FH is an autosomal dominant disease with defects in the gene for the LDL receptor. Patients presenting with severe forms of hypercholesterolaemia should undergo family screening to detect other family members for therapy.2. Therapy of these disorders is directed towards aggressive management of hypercholesterolaemia with a goal LDL-C that depends on the overall coronary risk of the affected person.2. References. 1. Yeshurun D, Gotto AM. Southern Med J 1995;88(4):379– Expert Panel on Detection, Evaluation, and Treatment of High Blood Cholesterol in Adults. JAMA 2001:285;2486–2497. Adapted from Southern Med J 1995;88:379–391, with permission from Lippincott Williams & Wilkins. LDL – lipoproteiny o małej gęstości; IDL – lipoproteiny o pośredniej gęstości; VLDL – lipoproteiny o bardzo małej gęstości. (lipoproteiny o dużej gęstości(HDL) nię są uwzględnione w klasyfikacji Fredricksona) Yeshurun D, Gotto AM. Southern Med J 1995;88(4):379–391.")
5
Ryzyko ChNS a stężenie cholesterolu całkowitego
Badanie Framingham 150 125 100 Występowanie ChNS na 1000 osób 75 50 As of 1984, in most of northern Europe, North America, and other industrialized Caucasian societies, CHD is the number one cause of death. Cardiovascular disease is associated with increased levels of total cholesterol. Other risk factors include an increase in TC to HDL cholesterol ratio, hypertension, cigarette smoking, excess weight, elevated blood sugar levels, lack of exercise, stress, and electrocardiographic abnormalities. Intervention trials have shown that identifying and lowering these risk factors may help to reduce the subsequent rate of coronary heart disease, stroke, and other cardiovascular diseases.1 Reference Castelli WP. Epidemiology of coronary heart disease: The Framingham Study. Am J Med. 1984;76:4-12. 25 204 295 Stężenie cholesterolu całkowitego (mg/dL) Castelli WP. Am J Med. 1984;76:4-12.
 Castelli WP. Am J Med. 1984;76:4-12.")
6
Śmiertelność z powodu ChNS w zależność od stężenia cholesterolu całkowitego
Badanie MRFIT 4 3 3,42 Ryzyko względne śmierci 2 2,21 1,73 The Multiple Risk Factor Intervention Trial (MRFIT) measured serum cholesterol levels and long-term mortality in 356,222 men aged 35 to 57. The trial showed a continuous graded relationship of mortality relative risk versus cholesterol levels. CHD death rate in each quintile was continuous, graded, and strong regardless of risk factors such as history, hypertension, or smoking.1 Reference Stamler J, Wentworth D, Neaton JD. Is relationship between serum cholesterol and risk of premature death from coronary heart disease continuous and graded? Findings in 356,222 primary screenees of the Multiple Risk Factor Intervention Trial (MRFIT). JAMA 1986;256: 1 n = (35-57 lat) 1,29 1 < 182 > 244 Stężenie cholesterolu całkowitego (mg/dL) Stamler J, et al. JAMA. 1986;256:
 measured serum cholesterol levels and long-term mortality in 356,222 men aged 35 to 57. The trial showed a continuous graded relationship of mortality relative risk versus cholesterol levels. CHD death rate in each quintile was continuous, graded, and strong regardless of risk factors such as history, hypertension, or smoking.1. Reference. Stamler J, Wentworth D, Neaton JD. Is relationship between serum cholesterol and risk of premature death from coronary heart disease continuous and graded Findings in 356,222 primary screenees of the Multiple Risk Factor Intervention Trial (MRFIT). JAMA 1986;256: n = (35-57 lat) 1, < > 244. Stężenie cholesterolu całkowitego (mg/dL) Stamler J, et al. JAMA. 1986;256:")
7
Cholesterol - modyfikowalny czynnik ryzyka ChNS
W USA Ponad 100 milionów dorosłych ma stężenie TCh 200 mg/dL1 Ponad 40 milionów dorosłych ma stężenie TCh levels 240 mg/dL1 Spadek stężenie TCh o 10% = redukcja ryzyka śmierci z powodu ChNS o 15% i redukcja śmiertelności całkowitej o 11% w metaanalizie 38 badań ze statynami2 LDL jako główny cel zapobiegania ChNS3 Rodzaj i intensywność interwencji zależą od całkowitego ryzyka CV 3 It has been estimated that in the United States more than 100 million adults have total cholesterol levels of 200 mg/dL and 40 million adults have levels of 240 mg/dL.1 Early lipid intervention trials have demonstrated that a reduction in total cholesterol results in a reduction in the incidence of CV events. In addition, a recent meta-analysis of 38 statin trials has shown that for every 10% reduction in total cholesterol, CHD mortality risk is reduced by 15% and total mortality risk is reduced by 11%.2 LDL cholesterol has been recognized as a prime target for lipid intervention to prevent CHD.3 Jacobson and colleagues analyzed NHANES III data and found that approximately 28.4 million Americans required drug therapy according to ATP II guidelines while only an estimated 4.5 million were receiving drug therapy.4 According to ATP III guidelines an estimated 36.5 million Americans require drug therapy.5 The intensity of intervention depends not only on raised cholesterol or LDL cholesterol but also on the presence of a number of other CV risk factors.3 References American Heart Association Heart and Stroke Statistical Update. Gould AL, Rossouw JE, Santanello NC, et al. Cholesterol reduction yields clinical benefit: impact of statin trials. Circulation. 1998;97: Expert Panel on Detection, Evaluation, and Treatment of High Blood Cholesterol in Adults. Executive Summary of the National Cholesterol Education Program (NCEP) Expert Panel on Detection, Evaluation, and Treatment of High Blood Cholesterol in Adults (Adult Treatment Panel III) JAMA. 2001;285: Jacobson TA, Griffiths GG, Varas C, et al. Impact of evidence-based "clinical judgment" on the number of American adults requiring lipid-lowering therapy based on updated NHANES III data. National Health and Nutrition Examination Survey. Arch Intern Med. 2000;160: NHLBI. Adult Treatment Panel III (ATP III) Guidelines Slide Show. Available at: Accessed October 25, 2001. 1. American Heart Association Heart and Stroke Statistical Update 2. Gould AL, et al. Circulation. 1998;97: 3. NCEP, Adult Treatment Panel III. JAMA. 2001;285:
 Expert Panel on Detection, Evaluation, and Treatment of High Blood Cholesterol in Adults (Adult Treatment Panel III) JAMA. 2001;285: Jacobson TA, Griffiths GG, Varas C, et al. Impact of evidence-based clinical judgment on the number of American adults requiring lipid-lowering therapy based on updated NHANES III data. National Health and Nutrition Examination Survey. Arch Intern Med. 2000;160: NHLBI. Adult Treatment Panel III (ATP III) Guidelines Slide Show. Available at: Accessed October 25, American Heart Association Heart and Stroke Statistical Update Gould AL, et al. Circulation. 1998;97: NCEP, Adult Treatment Panel III. JAMA. 2001;285:")
8
EUROASPIRE I and II Group. Lancet. 2001; 357: 995-1001.
Występowanie czynników ryzyka u pacjentów z potwierdzoną ChNS - badanie EUROASPIRE n=6948 Hipercholesterolemia (TCh ≥194 mg/dl / 5mmol/l) Nadciśnienie tętnicze (SBP ≥140 mm Hg i/lub DBP ≥90 mm Hg Otyłość (BMI >30 kg/m2) Palenie papierosów 58,8% 53,9% 32,8% 20,8% EUROASPIRE I and II Group. Lancet. 2001; 357:
 Nadciśnienie tętnicze. (SBP ≥140 mm Hg i/lub DBP ≥90 mm Hg. Otyłość. (BMI >30 kg/m2) Palenie papierosów. 58,8% 53,9% 32,8% 20,8% EUROASPIRE I and II Group. Lancet. 2001; 357:")
9
ddd

10
Znaczenie farmakoterapii w prewencji wtórnej
RRR Częstość zdarzeń CV Bez farmakoterapii 8% ASA 25% 6% -blokery 4,5% Statyny 30% 3,0% ACE-inhibitory 2,3% ŁĄCZNA WZGLĘDNA REDUKCJA RYZYKA 75% Zdarzenia CV = Zgony CV, zawały serca i udary mózgu Yusuf, S. Two decades of progress in preventing vascular disease. Lancet 2002; 360: 2-3.

11
Zalecenia odnośnie rozpoznawania hiperlipidemii
Wytyczne European Society of Cardiology Cardiovascular Disease Prevention in Clinical Practice Estimation of ten-year risk of fatal cardiovascular disease in Europe: the SCORE project Wytyczne National Heart, Lung, and Blood Institute/National Institutes of Health Detection, Evaluation, and Treatment of High Blood Cholesterol in Adults (Adult Treatment Panel III)
")
13
Wg ESC w populacji ogólnej ze zwiększonym ryzykiem sercowo-naczyniowym wiążą się
TCH ³190 mg/dl LDL ³115 mg/dl TG ³150 mg/dl HDL M <40 mg/dl; K <45 mg/dl

14
Stężenia LDL, HDL, TCH,, TG wg ATP III [mg/dl]
<100 Optymalne Zbliżone do optymalnego Granicznie wysokie Wysokie 190 Bardzo wysokie HDL <40 Niskie 60 Wysokie TCH <200 Pożądane 200–239 Granicznie wysokie 240 Wysokie TG <150 Prawidłowe Granicznie wysokie Wysokie Bardzo wysokie
![Stężenia LDL, HDL, TCH,, TG wg ATP III [mg/dl]](http://slideplayer.pl/slide/818069/2/images/14/St%C4%99%C5%BCenia+LDL%2C+HDL%2C+TCH%2C%2C+TG+wg+ATP+III+%5Bmg%2Fdl%5D.jpg "<100 Optymalne Zbliżone do optymalnego Granicznie wysokie Wysokie. 190 Bardzo wysokie. HDL. <40 Niskie. 60 Wysokie. TCH. <200 Pożądane. 200–239 Granicznie wysokie. 240 Wysokie. TG. <150 Prawidłowe Granicznie wysokie Wysokie. 500 Bardzo wysokie.")
15
Kategorie pacjentów wg ryzyka choroby wieńcowej - ESC
Osoby z rozpoznaną chorobą wieńcową, miażdżycą tętnic obwodowych lub chorobą naczyń mózgowych Osoby bez objawów obciążone zwiększonym ryzykiem w/w chorób, jeśli: Ryzyko zgonu z powodu licznych czynników ryzyka ³5% - karta SCORE Silny pojedynczy czynnik ryzyka: TCH ³320mg/dl, LDL ³240mg/dl, SBP ³180mm Hg lub DBP ³110 mm Hg Cukrzyca typu 2 lub cukrzyca typu 1 z mikroalbuminurią Bliscy krewni: Chorych, u których wcześnie rozwinęła się jawna klinicznie choroba wieńcowa Osób bez objawów choroby, lecz obciążonych dużym ryzykiem Inne osoby pozostające pod rutynową opieką lekarską

16
Osoby z chorobą wieńcową, miażdżycą tętnic kończyn dolnych lub chorobą naczyń mózgowych obciążone są dużym ryzykiem sercowo-naczyniowym (³5%) i powinny być objęte programem profilaktyki wtórnej. Cele profilaktyki wtórnej u w/w pacjentów oraz osób chorych na cukrzycę bez choroby wieńcowej Zmniejszenie stężenie TCH<175 mg/dl (opcja <155 mg/dl ) i LDL<100 mg/dl (opcja <80 mg/dl ) Obniżenie ciśnienia tętniczego <140/90 (u chorych na cukrzycę <130/80) W przypadku nadwagi lub otyłości zmniejszenie wagi ciała o ³10%
 i LDL<100 mg/dl (opcja <80 mg/dl ) Obniżenie ciśnienia tętniczego <140/90 (u chorych na cukrzycę <130/80) W przypadku nadwagi lub otyłości zmniejszenie wagi ciała o ³10%")
18
pacjentów Obserwacja 3 mln pacjento-lat 700 zgonów CV

19
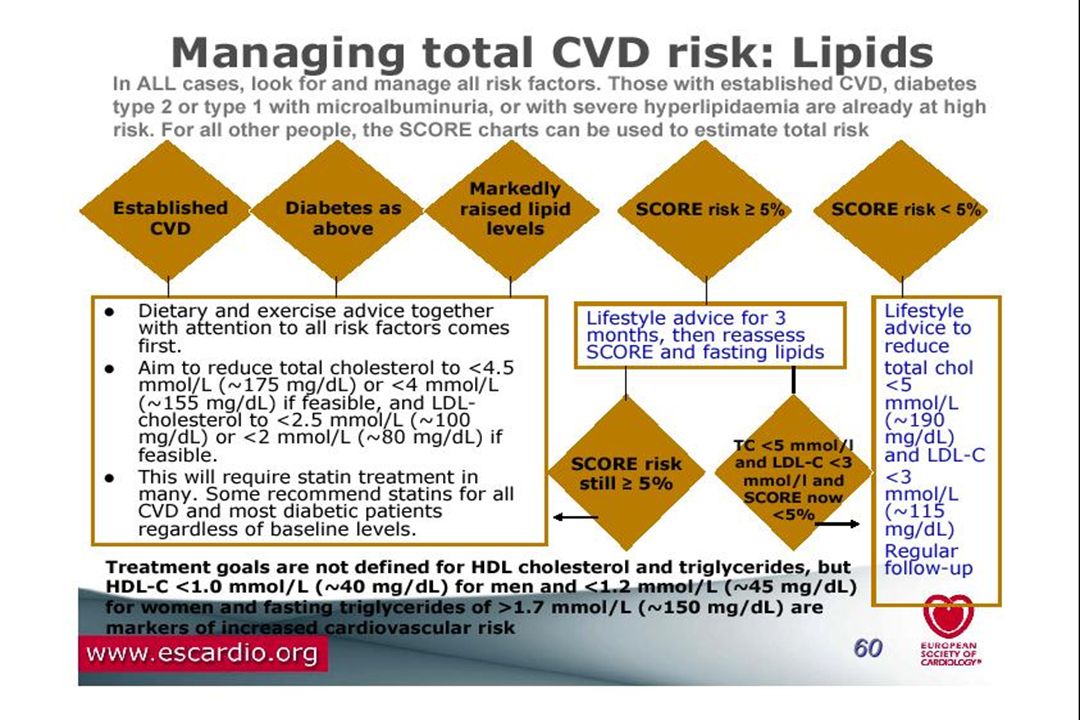
Algorytm postępowania w hipercholesterolemii u osób bez klinicznie jawnej choroby sercowo-naczyniowej wg ESC Oceń ryzyko zgonu z przyczyn sercowo-naczyniowych u użyciem karty SCORE - Ryzyko <5% - TCH ³190 mg/dl - Ryzyko ³5% - TCH ³190 mg/dl Zalecenie zmiany stylu życia w celu zmniejszenia TCH <190 mg/dl i LDL <115 mg/dl Wizyty kontrolne przynajmniej co 5 lat Oznacz profil lipidowy osocza na czczo Zalecenie zmiany stylu życia przez 3 miesiące i po tym czasie ponowny pomiar stężenia lipidów - TCH <190 mg/dl - LDL <115 mg/dl - TCH ³190 mg/dl i/lub - LDL ³115 mg/dl - Utrzymuj zalecenia odnośnie stylu życia Wizyty kontrolne co roku Jeśli ryzyko całkowite nadal ³5% rozważ stosowanie leków w celu zmniejszenia TCH <175 mg/dl i LDL <100 mg/dl - Utrzymuj zalecenia odnośnie stylu życia Rozpocznij leczenie farmakologiczne

20
Ekwiwalenty choroby wieńcowej wg ATP III
Inne formy miażdżycy (miażdżyca tętnic kończyn dolnych, tętniak aorty brzusznej, objawowe zwężenia tętnic szyjnych) Cukrzyca 10-letnie ryzyko zawału serca i zgonu sercowego wg skali Framingham >20%
 Cukrzyca. 10-letnie ryzyko zawału serca i zgonu sercowego wg skali Framingham >20%")
21
Porównanie docelowych wartości lipidogramu dla grup dużego ryzyka wg ESC i ATP III
TCH <175 mg/dl <200 mg/dl LDL <100 mg/dl HDL Brak >40 mg/dl TG <150 mg/dl

22
Docelowe stężenie LDL-C - nowelizacja ATP III
Populacja pacjentów Cel terapeutyczny Wszyscy pacjenci bardzo dużego ryzyka Choroba naczyniowa-sercowa współistniejąca z kilkoma czynnikami ryzyka lub zespołem metabolicznym, ostry zespół wieńcowy LDL-C <100 mg/dl Wszyscy pacjenci bardzo dużego ryzyka, gdy LDL-C <100mg/dl Opcjonalne leczenie do osiągnięcia LDL-C <70 mg/dl Pacjenci dużego ryzyka Obecność choroby wieńcowej lub ekwiwalentu choroby wieńcowej (np. cukrzycy) - 10-letnie ryzyko w skali Framingham >20% Zawsze włączenie leczenia do osiągnięcia Circulation. 2004; 110:
 - 10-letnie ryzyko w skali Framingham >20% Zawsze włączenie leczenia do osiągnięcia. Circulation. 2004; 110:")
23
Docelowe stężenie LDL-C - nowelizacja ATP III c.d.
Populacja pacjentów Cel terapeutyczny Pacjenci dużego ryzyka, gdy LDL-C mg/dl Obecność choroby wieńcowej lub ekwiwalentu choroby wieńcowej (np. cukrzycy) - 10-letnie ryzyko w skali Framingham >20% Zawsze włączenie leczenia do osiągnięcia LDL-C <100 mg/dl Pacjenci umiarkowanie dużego ryzyka, Obecność co najmniej dwóch czynników ryzyka i ryzyko wg skali Framingham 10-20% LDL-C <130 mg/dl opcjonalnie leczenie dla osiągnięcia Pacjenci umiarkowanie dużego ryzyka, gdy LDL-C mg/dl Circulation. 2004; 110:
 - 10-letnie ryzyko w skali Framingham >20% Zawsze włączenie leczenia do osiągnięcia. LDL-C <100 mg/dl. Pacjenci umiarkowanie dużego ryzyka, Obecność co najmniej dwóch czynników ryzyka i ryzyko wg skali Framingham 10-20% LDL-C <130 mg/dl opcjonalnie leczenie dla osiągnięcia. Pacjenci umiarkowanie dużego ryzyka, gdy LDL-C mg/dl. Circulation. 2004; 110:")
24
Ryzyko ChNS oszacowane na podstawie stężeń HDL i LDL w badaniu Framingham
Ryzyko względne ChNS As shown in this slide, the risk associated with HDL is independent of the risk associated with LDL. At any level of LDL, a decrease in HDL increases the risk of CHD. HDL [mg/dL] LDL [mg/dL] AJC 2001; 88(suppl): 9N-13N
: 9N-13N.")
25
Zależność między ryzykiem ChNS a stężeniami HDL i TG w badaniu PROCAM
128 94 140 120 100 Zdarzenia wieńcowe (wskaźnik/1 000 osób/6 lat) 80 60 46 Niski HDL (<35 mg/dL) 24 40 Further, the PROCAM study showed that the risk associated with HDL is independent of the risk associated with triglycerides. 20 Wysoki HDL (>35 mg/dL) Niskie TG Wysokie TG (<200 mg/dL) (>200 mg/dL) AJC 2001; 88(suppl): 9N-13N
 Niski HDL (<35 mg/dL) Further, the PROCAM study showed that the risk associated with HDL is independent of the risk associated with triglycerides. 20. Wysoki HDL (>35 mg/dL) Niskie TG. Wysokie TG. (<200 mg/dL) (>200 mg/dL) AJC 2001; 88(suppl): 9N-13N.")
26
CHRC Vascular Protection Registry 278 lekarzy prowadzących rekrutację
5,091 pacjentów 278 lekarzy prowadzących rekrutację Czas trwania 2001 – 2004 Newfoundland 12 MDs n=151 New Brunswick 12 MDs n=164 British Columbia 39 MDs n=750 Saskatchewan 18 MDs n=272 Quebec 65 MDs n=1025 To-date, approximately 3,400 patients from 186 physicians have been enrolled in the Canadian Heart Research Centre (CHRC)-coordinated Vascular Protection (VP) Registry from December ; the number of physicians and total number of patients enrolled in each province are listed. Alberta 16 MDs n=160 Manitoba 16 MDs n=615 Ontario 89 MDs N=1752 P.E.I Nova Scotia 11 MDs n=202 Wiek (lata) 66 (57;73) Mężczyźni 65% Cukrzyca 57,3% Choroba wieńcowa 56,8%
-coordinated Vascular Protection (VP) Registry from December ; the number of physicians and total number of patients enrolled in each province are listed. Alberta 16 MDs. n=160. Manitoba 16 MDs. n=615. Ontario 89 MDs. N=1752. P.E.I. Nova Scotia 11 MDs. n=202. Wiek (lata) 66 (57;73) Mężczyźni 65% Cukrzyca 57,3% Choroba wieńcowa 56,8%")
27
Odsetek chorych, którzy osiągnęli cele leczenia
% pacjentów 100 79 80 54 55 49 60 47 40 20 SBP < 130 DBP < 80 LDL-C < 100 TC/HDL < 4,0 A1C < 7%

28
Badanie CALIPSO 90 80 70 60 50 40 30 20 10 All patients
All patients High-risk patients 81% 57% % of Patients Not at Goal 36% 27% This slide illustrates the proportions of CALIPSO patients that did not achieve their LDL-C goal (including the entire population as shown on the previous slide with a 27% rate of failure to reach respective targets as well as the subgroup of high-risk patients with a 36% rate of failure to to reach the risk-associated 2.5 mmol/L target ). The set of bars on the right side of this graph show the proportions of CALIPSO patients that would have failed to reach LDL-C goal based on the NCEP ATP III 2004 update (with the optional 1.8 mmol/L LDL-C target for high-risk patients). As shown, 57% of all patients and 81% of high-risk patients would not be at goal based on this optional target. Reference: Bourgault C, Davignon J, Fodor G, et al. Statin therapy in Canadian patients with hypercholesterolemia: the CALIPSO study. Can J Cardiol 2005 (submitted December 2004). % Not at Goal (High-risk target: 2.5 mmol/L) % Not at Goal (High-risk target: 1.8 mmol/L) Bourgault C. et al, Can J Cardiol 2005; 21(13):
. The set of bars on the right side of this graph show the proportions of CALIPSO patients that would have failed to reach LDL-C goal based on the NCEP ATP III 2004 update (with the optional 1.8 mmol/L LDL-C target for high-risk patients). As shown, 57% of all patients and 81% of high-risk patients would not be at goal based on this optional target. Reference: Bourgault C, Davignon J, Fodor G, et al. Statin therapy in Canadian patients with hypercholesterolemia: the CALIPSO study. Can J Cardiol 2005 (submitted December 2004). % Not at Goal (High-risk target: 2.5 mmol/L) % Not at Goal (High-risk target: 1.8 mmol/L) Bourgault C. et al, Can J Cardiol 2005; 21(13):")
29
Wybrane badania statynowe w prewencji pierwotnej i wtórnej
Trial Baseline LDL-C (mmol/L) On-Treatment LDL-C (% reduction) Statin Event* Rate (%) Placebo Event* Rate (%) RRR (%) ARR NNT 4S 4.9 3.2 (35) 19.4 28.0 34 8.6 12 LIPID 3.9 2.9 (25**) 12.3 15.9 24 3.6 28 CARE 2.5 (32) 10.2 13.2 3.0 HPS ~3.3 ~2.3 (29**) 19.9 25.4 5.5 18 WOSCOPS 4.1 (26) 5.3 7.5 29 2.2 46 AFCAPS 3.0 (25) 3.5 37 2.0 50 Clinical Trials Of Statins In Primary And Secondary Prevention A substantial body of evidence supports the use of lipid-lowering treatment in the prevention of CAD morbidity and mortality. Several statin trials, beginning with 4S in 1994, have evaluated the effects of statins on clinical event end points. As shown in this slide, these trials provided robust and consistent evidence of the benefits of intervention across a broad range of patient cohorts. Accordingly, the NCEP ATP guidelines recommended statins for primary and secondary prevention of CAD. 4S = Scandinavian Simvastatin Survival Study; AFCAPS = Air Force Coronary Atherosclerosis Prevention Study; CARE = Cholesterol and Recurrent Events study; CHD = coronary heart disease; LIPID = Long-term Intervention with Pravastatin in Ischaemic Disease study; MI = myocardial infarction. *Nonfatal MI or CHD death in WOSCOPS, CARE, LIPID; nonfatal or fatal MI, unstable angina, or sudden cardiac death in AFCAPS; nonfatal MI, coronary death, or resuscitated cardiac arrest in 4S; major vascular events (total CHD, total stroke, revascularizations) in HPS; **Versus placebo.
 On-Treatment LDL-C. (% reduction) Statin Event* Rate (%) Placebo Event* Rate (%) RRR. (%) ARR. NNT. 4S (35) LIPID (25**) CARE. 2.5 (32) HPS. ~3.3. ~2.3 (29**) WOSCOPS. 4.1 (26) AFCAPS. 3.0 (25) Clinical Trials Of Statins In Primary And Secondary Prevention. A substantial body of evidence supports the use of lipid-lowering treatment in the prevention of CAD morbidity and mortality. Several statin trials, beginning with 4S in 1994, have evaluated the effects of statins on clinical event end points. As shown in this slide, these trials provided robust and consistent evidence of the benefits of intervention across a broad range of patient cohorts. Accordingly, the NCEP ATP guidelines recommended statins for primary and secondary prevention of CAD. 4S = Scandinavian Simvastatin Survival Study; AFCAPS = Air Force Coronary Atherosclerosis Prevention Study; CARE = Cholesterol and Recurrent Events study; CHD = coronary heart disease; LIPID = Long-term Intervention with Pravastatin in Ischaemic Disease study; MI = myocardial infarction. *Nonfatal MI or CHD death in WOSCOPS, CARE, LIPID; nonfatal or fatal MI, unstable angina, or sudden cardiac death in AFCAPS; nonfatal MI, coronary death, or resuscitated cardiac arrest in 4S; major vascular events (total CHD, total stroke, revascularizations) in HPS; **Versus placebo.")
30
Średnie stężenie LDL-cholesterolu w trakcie leczenia (mg/dl)
Zależność między występowaniem ostrych zespołów wieńcowych i stężeniem cholesterolu LDL w badaniach statynowych 30 Prewencja Wtórna 4S-Pl 25 4S 20 Częstość zdarzeń sercowo-naczyniowych [%] LIPID-Pl 15 CARE CARE-Pl LIPID WOSCOPS-Pl 10 Prewencja Pierwotna WOSCOPS AFCAPS 5 AFCAPS-Pl Slide IV/18 The relationship between statin therapy and outcome is a function of the on-trial LDL-C level. A composite plot of major clinical trials using statins demonstrates this important clinical point. There is greater absolute benefit when these treatments are applied for secondary prevention.119 Although primary prevention appears less striking, the percentage reduction in primary trials 111,120 was greater than that in secondary trials The benefits of therapy beyond lower limits of LDL-C shown on this slide are currently being evaluated in ongoing clinical trials. 70 90 (2.3 mmol/L) 110 130 150 (3.9 mmol/L) 170 190 (5.4 mmol/L) 210 Średnie stężenie LDL-cholesterolu w trakcie leczenia (mg/dl) N Engl J Med 1995;333: ; Lancet 1995;345: ; JAMA 1996;335: ; JAMA 1998;279: ; N Engl J Med 1998;339:
 (3.9 mmol/L) (5.4 mmol/L) 210. Średnie stężenie LDL-cholesterolu w trakcie leczenia (mg/dl) N Engl J Med 1995;333: ; Lancet 1995;345: ; JAMA 1996;335: ; JAMA 1998;279: ; N Engl J Med 1998;339:")
31
Redukcja LDL z użyciem statyn zmniejsza progresję miażdżycy
0,06 Placebo Drug therapy 0,05 PLAC I REGRESS CCAIT 0,04 LCAS Zmniejszenie MLD [mm/rok] 0,03 PLAC I MARS MAAS CCAIT 0,02 Angiographic trials in patients with elevated LDL-C ranging from mild to severe have demonstrated consistent benefit in the progression of coronary artery disease (the difference between minimum lumen diameter [MLD] decrease in drug [Rx] and placebo [PL] patients) with statin therapy.1 Fluvastatin was used in: LCAS (Lipoprotein and Coronary Atherosclerosis Study). Herd JS, Ballantyne CM, Farmer JA et al. Am J Cardiol 1997;80: Lovastatin was used in: CCAIT (Canadian Coronary Atherosclerosis Intervention Trial). Waters D, Higginson L, Gladstone P et al. Circulation 1994;89: MARS (Monitored Atherosclerosis Regression Study). Blankenhorn DH, Azen SP, Kramsch DM et al. Ann Intern Med 1993;119: Pravastatin was used in: PLAC I (Pravastatin Limitation of Atherosclerosis in the Coronary Arteries). Pitt B, Mancini GBJ, Ellis SG et al. J Am Coll Cardiol 1995;26: REGRESS (Regression Growth Evaluation Statin Study). Jukema JW, Bruschke AVG, van Boven et al. Circulation 1995;91: Simvastatin was used in: MAAS (Multicentre Anti-Atheroma Study). The MAAS Investigators. Lancet 1994;344: Reference Ballantyne CM. Am J Cardiol 1998;82:3Q–12Q. Adapted from Am J Cardiol 1998;82:3Q–12Q, with permission from Excerpta Medica Inc. MARS REGRESS MAAS 0,01 LCAS 70 (1,8) 90 (2,3) 110 (2,8) 130 (3,4) 150 (3,9) 170 (4,4) 190 (5,0) Stężenie LDL w trakcie leczenia mg/dL (mmol/L) MLD - minimalne świtało naczynia Ballantyne CM et al. Am J Cardiol 1998;82:3Q–12Q.
 with statin therapy.1. Fluvastatin was used in: LCAS (Lipoprotein and Coronary Atherosclerosis Study). Herd JS, Ballantyne CM, Farmer JA et al. Am J Cardiol 1997;80: Lovastatin was used in: CCAIT (Canadian Coronary Atherosclerosis Intervention Trial). Waters D, Higginson L, Gladstone P et al. Circulation 1994;89: MARS (Monitored Atherosclerosis Regression Study). Blankenhorn DH, Azen SP, Kramsch DM et al. Ann Intern Med 1993;119: Pravastatin was used in: PLAC I (Pravastatin Limitation of Atherosclerosis in the Coronary Arteries). Pitt B, Mancini GBJ, Ellis SG et al. J Am Coll Cardiol 1995;26: REGRESS (Regression Growth Evaluation Statin Study). Jukema JW, Bruschke AVG, van Boven et al. Circulation 1995;91: Simvastatin was used in: MAAS (Multicentre Anti-Atheroma Study). The MAAS Investigators. Lancet 1994;344: Reference. Ballantyne CM. Am J Cardiol 1998;82:3Q–12Q. Adapted from Am J Cardiol 1998;82:3Q–12Q, with permission from Excerpta Medica Inc. MARS. REGRESS. MAAS. 0,01. LCAS. 70. (1,8) 90. (2,3) 110. (2,8) 130. (3,4) 150. (3,9) 170. (4,4) 190. (5,0) Stężenie LDL w trakcie leczenia mg/dL (mmol/L) MLD - minimalne świtało naczynia. Ballantyne CM et al. Am J Cardiol 1998;82:3Q–12Q.")
32
Wpływ redukcji LDL-C na objętość blaszki miażdżycowej
20 Both Treatment Groups (n=502) 15 10 5 Zmiana objętości blaszki mm3 -5 Linear regression analysis for both treatment groups showed an inverse relationship between percentage reduction in LDL-C level and progression of atherosclerotic disease. These data illustrate the benefits of intensive lipid lowering and show that, regardless of the agent used, an LDL-C reduction of at least 50% was required to halt progression. -10 -15 -80 -70 -60 -50 -40 -30 -20 -10 10 20 Zmiana LDL-C [%] Bez względu na rodzaj użytego preparatu zatrzymanie postępu miażdżycy wymagało obniżenia stężenia LDL-C ro co najmniej 50%.
 Zmiana objętości blaszki mm Linear regression analysis for both treatment groups showed an inverse relationship between percentage reduction in LDL-C level and progression of atherosclerotic disease. These data illustrate the benefits of intensive lipid lowering and show that, regardless of the agent used, an LDL-C reduction of at least 50% was required to halt progression Zmiana LDL-C [%] Bez względu na rodzaj użytego preparatu zatrzymanie postępu miażdżycy wymagało obniżenia stężenia LDL-C ro co najmniej 50%.")
33
REGUŁA ROBERTSA ATOR SIMWA LOWA PRAWA FLUWA CHOL LDL TG - 10 mg 20 mg
- 22% - 27% -10 /15% 80 mg - 34% % 80 XL - 32% - 41% -15/25% - 37% - 48% -20/30% ... - 42% - 55% - 25/35%

34
Cele leczenia hipolipemizującego
Twarde punkty końcowe Śmiertelność całkowita Śmiertelność sercowo-naczyniowa Zawały serca Złożone punkty końcowe MACE Zastępczne punkty końcowe Zmiany lipidogramu Objętość blaszki miażdżycowej IMT

36
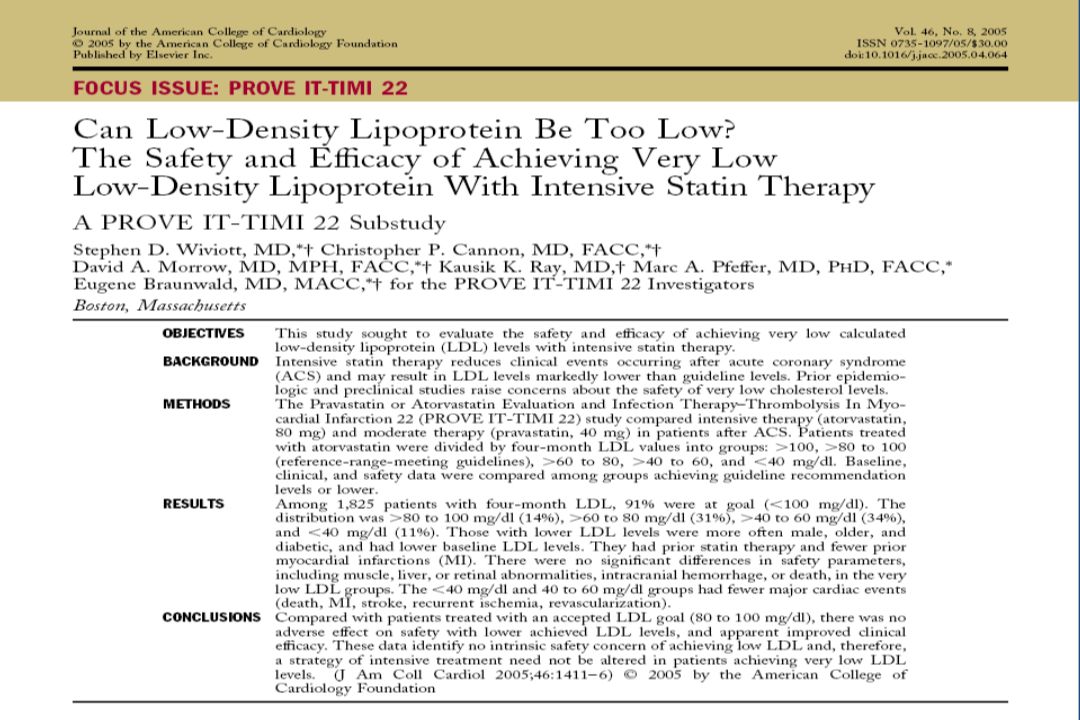
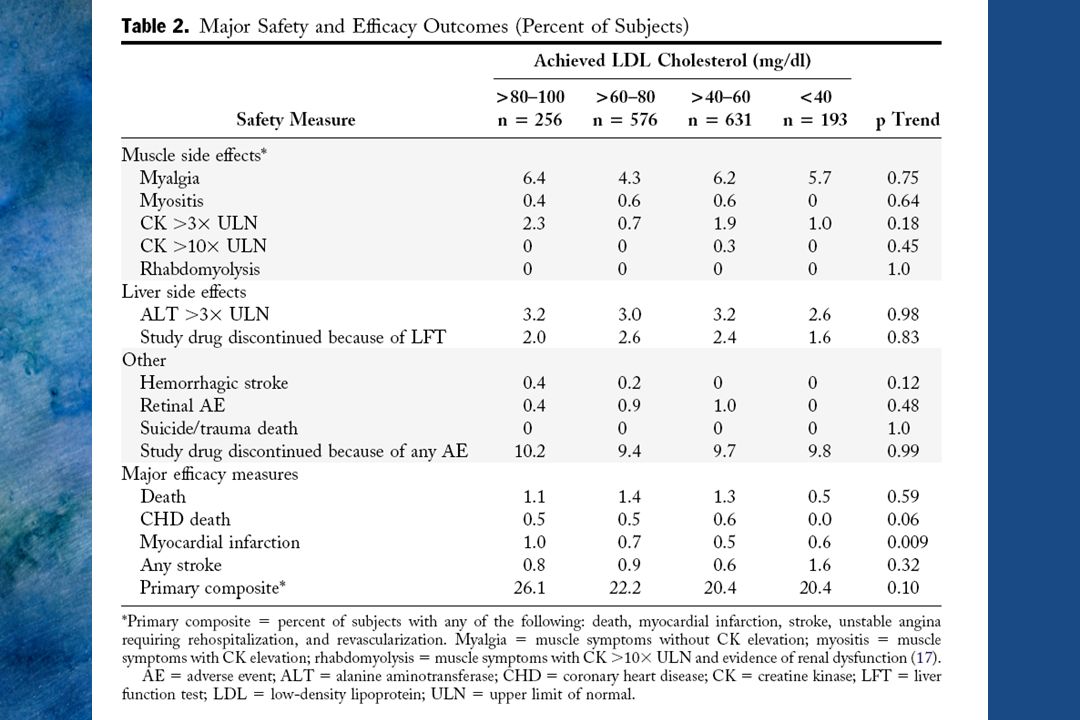
1O endpoint: death, MI, stroke, recurrent ischaemia, revascularization

39
27 548 pacjentów z 4 randomizowanych badań (TNT, IDEAL, PROVE IT-TIMI-22, A-to-Z)
Oceniane łącznie redukcja ryzyka zgonu z powodu choroby wieńcowej i redukcja ryzyka zawału serca o 16% Bez wpływu na śmiertelność całkowitą oraz śmiertelność z innych powodów niż choroby sercowo-naczyniowe Trend ku redukcji śmiertelności sercowo-naczyniowej o 12% (p=0,054)
")
40
Nowe możliwości leczenia Terapia łączona - statyna z czym ?
Redukcja LDL-C inhibitor wchłaniania cholesterolu – Ezetimib/Ezetrol® Wzrost HDL Niacina/Niaspan® /Fibrat Redukcja TG Fibraty (fenofibrat)/ Niacina/Niaspan®
/ Niacina/Niaspan®")
41
Ezetimib + Statyna Wpływ na LDL-C łącznie z różnymi statynami
Lowastatyna Mono + ezetimib (n=220) (n=192) Prawastatyna Mono + ezetimib (n=205) (n=204) Simwastatyna Mono + ezetimib (n=263) (n=274) Atorwastatyna Mono + ezetimib (n=248) (n=255) 0% –10% –20% Mean % Change in LDL-C From Untreated Baseline –30% –25% –25% –40% Ezetimibe plus a statin provided significant additional LDL-C lowering, compared with statin monotherapy. Ezetimibe increased LDL-C lowering efficacy when it was added to any statin tested. References: Ballantyne CM et al for the Ezetimibe Study Group. Effect of ezetimibe coadministered with atorvastatin in 628 patients with primary hypercholesterolemia: a prospective, randomized, double-blind trial. Circulation 2003; 107: Davidson MH et al for the Ezetimibe Study Group. Ezetimibe coadministered with simvastatin in patients with primary hypercholesterolemia. J Am Coll Cardiol 2002;40(12): Melani L et al for the Ezetimibe Study Group. Efficacy and safety of ezetimibe coadministered with pravastatin in patients with primary hpercholesterolemia: A prospective, randomized, double-blind trial. Eur Heart J 2003;24: Kerzner B et al for the Ezetimibe Study Group. Efficacy and safety of ezetimibe coadministered with lovastatin in primary hypercholesterolemia. Am J Cardiol 2003;91(4): –36% –40%* –39%* –50% –44% –51%* –60% –56%* Lowastatyna Simwastatyna Ezetimib + Statyna –70% Prawastatyna Atorwastatyna *p < 0.01 dla ezetimib + statyna vs sama statyna. Ballantyne CM et al. Circulation 2003; 107: Melani L et al. Eur Heart J 2003;24: Davidson MH et al. J Am Coll Cardiol 2002;40(12): Kerzner B et al. Am J Cardiol 2003;91(4)
 (n=192) Prawastatyna. Mono + ezetimib. (n=205) (n=204) Simwastatyna. Mono + ezetimib. (n=263) (n=274) Atorwastatyna. Mono + ezetimib. (n=248) (n=255) 0% –10% –20% Mean % Change in LDL-C. From Untreated Baseline. –30% –25% –25% –40% Ezetimibe plus a statin provided significant additional LDL-C lowering, compared with statin monotherapy. Ezetimibe increased LDL-C lowering efficacy when it was added to any statin tested. References: Ballantyne CM et al for the Ezetimibe Study Group. Effect of ezetimibe coadministered with atorvastatin in 628 patients with primary hypercholesterolemia: a prospective, randomized, double-blind trial. Circulation 2003; 107: Davidson MH et al for the Ezetimibe Study Group. Ezetimibe coadministered with simvastatin in patients with primary hypercholesterolemia. J Am Coll Cardiol 2002;40(12): Melani L et al for the Ezetimibe Study Group. Efficacy and safety of ezetimibe coadministered with pravastatin in patients with primary hpercholesterolemia: A prospective, randomized, double-blind trial. Eur Heart J 2003;24: Kerzner B et al for the Ezetimibe Study Group. Efficacy and safety of ezetimibe coadministered with lovastatin in primary hypercholesterolemia. Am J Cardiol 2003;91(4): –36% –40%* –39%* –50% –44% –51%* –60% –56%* Lowastatyna. Simwastatyna. Ezetimib + Statyna. –70% Prawastatyna. Atorwastatyna. *p < 0.01 dla ezetimib + statyna vs sama statyna. Ballantyne CM et al. Circulation 2003; 107: Melani L et al. Eur Heart J 2003;24: Davidson MH et al. J Am Coll Cardiol 2002;40(12): Kerzner B et al. Am J Cardiol 2003;91(4)")
42
Toczące się badania kliniczne dotyczące ezetimibu i simwastatyny
Gotto AM and Farmer JA (2006) Drug Insight: the role of statins in combination with ezetimibe to lower LDL cholesterol Nat Clin Pract Cardiovasc Med 3: 664–672
 Drug Insight: the role of statins in combination with ezetimibe to lower LDL cholesterol. Nat Clin Pract Cardiovasc Med 3: 664–672.")
43
Refundacja - ezetimib na „P” Hipercholesterolemia LDL-C >130 mg/dl utrzymu-jąca się pomimo terapii statynami w przypadku: Przebytego zawału serca Przebytej rewaskularyzacji wieńcowej (PCI lub CABG) Przebytej rewaskularyzacji obwodowej Przebytej amputacji obwodowej z powodu miażdżycy Hipercholesterolemii rodzinnej
 Przebytej rewaskularyzacji obwodowej. Przebytej amputacji obwodowej z powodu miażdżycy. Hipercholesterolemii rodzinnej.")
44
Dodanie niacyny do statyny, gdy monoterapią nie osiągnięto celów leczenia
30 24% 23% 20 10 Zmiana wyrażona procentowo -10 -8% -8% -20 -18% This data is from a retrospective analysis of patients who were on a stable dose of statin before the addition on Niaspan. All patients were dyslipidemic; the clinical decision to initiate Niaspan was because of persistent dyslipidemia characterized either by LDL-C not at goal or low HDL-C with or without elevated TG. Patient data was analyzed on 66 patients who were on a stable dose of statin for at least 6 weeks before Niaspan was added. Patient characteristics were as follows:73% men (mean age 48.9 yr); 55% had CAD; 3% diabetes; 41% hypertensive. Statin treatment was as follows: 44 patients (out of 66) were on atorvastatin (of these, 7 were on 10 mg, 14 on 20 mg, 18 on 40 mg and 5 on 80 mg); 13 patients (out of 66) were on simvastatin (of these, 4 were on 10 mg, 3 on 20 mg and 6 on 40 mg; 8 patients (out of 66) were on pravastatin (of these, 5 were on 20 mg and 3 on 40 mg; 1 patient (out of 66) was on fluvastatin 40 mg. Baseline data (i.e. before the addition of Niaspan to a stable dose of statin) were as follows: LDL-C 3.4 mmol/L; HDL-C 1.0 mmol/L; TG 2.5 mmol/L. Safety analysis: No clinically important or statistically significant elevations in liver enzymes; no reports of muscle aches; no significant worsening of fasting glucose or uric acid levels. Reference: Wolfe ML, et al. Am J Cardiol 2001;87: -23% -30 -24% -30% -40 TC LDL HDL TG 1g NIASPAN (n=66) 2g NIASPAN (n=29) Wolfe et.al. Am J Cardiol 2001; 87:
; 55% had CAD; 3% diabetes; 41% hypertensive. Statin treatment was as follows: 44 patients (out of 66) were on atorvastatin (of these, 7 were on 10 mg, 14 on 20 mg, 18 on 40 mg and 5 on 80 mg); 13 patients (out of 66) were on simvastatin (of these, 4 were on 10 mg, 3 on 20 mg and 6 on 40 mg; 8 patients (out of 66) were on pravastatin (of these, 5 were on 20 mg and 3 on 40 mg; 1 patient (out of 66) was on fluvastatin 40 mg. Baseline data (i.e. before the addition of Niaspan to a stable dose of statin) were as follows: LDL-C 3.4 mmol/L; HDL-C 1.0 mmol/L; TG 2.5 mmol/L. Safety analysis: No clinically important or statistically significant elevations in liver enzymes; no reports of muscle aches; no significant worsening of fasting glucose or uric acid levels. Reference: Wolfe ML, et al. Am J Cardiol 2001;87: % % -30% -40. TC. LDL. HDL. TG. 1g NIASPAN (n=66) 2g NIASPAN (n=29) Wolfe et.al. Am J Cardiol 2001; 87:")
45
(BADANIE SAFARI) SIMWASTATYNĄ Z FENOFIBRATEM
EFEKTYWNOŚĆ I TOLERANCJA TERAPII SKOJARZONEJ SIMWASTATYNĄ Z FENOFIBRATEM W LECZENIU HYPERLIPIDEMII MIESZANEJ (BADANIE SAFARI) Scott M. Grundy, MD, PhD, Gloria L. Vega, PhD, Zhong Yuan, MD, PhD, Wendy P. Battisti, PhD, William E. Brody, MS and Joanne Palmisano, MD
 Scott M. Grundy, MD, PhD, Gloria L. Vega, PhD, Zhong Yuan, MD, PhD, Wendy P. Battisti, PhD, William E. Brody, MS and Joanne Palmisano, MD.")
46
ZMIANY POZIOMU LIPIDÓW W PORÓWNANIU DO WARTOŚCI WYJŚCIOWYCH
TG VLDL-C Non- HDL-C LDL-C HDL-C

47
W PORÓWNANIU DO WARTOŚCI WYJŚCIOWYCH
ZMIANY SUBFRAKCJI LDL W PORÓWNANIU DO WARTOŚCI WYJŚCIOWYCH Simwastatyna 20 mg/dzień + FENOFIBRAT 160 mg/dzień Simwastatyna 20mg/dzień Simwastatyna 20 mg/dzień + FENOFIBRAT 160 mg/dzień Simwastatyna 20mg/dzień POZIOM WYJŚCIOWY 12 TYDZIEŃ

48
Terapia skojarzona simwastatyną i fenofibratem
w porównaniu do monoterapii simwastatyną 20 mg u pacjentów z hyperlipidemią mieszaną zaowocowała dodatkową poprawą PARAMETRÓW LIPIDOWYCH oraz okazała się DOBRZE TOLEROWANA. Wniosek: Terapia skojarzona simwastatyną i fenofibratem jest korzystną opcją terapeutyczną w leczeniu hyperlipidemii mieszanej 2005 by Excerpta Medica Inc. (Am. J Cardiol 2005; 95: )
")
50
Canadian Fitness Craze

51
Dziękuję za uwagę