Pobierz prezentację
Pobieranie prezentacji. Proszę czekać

1
Kardiologia geriatryczna
Tomasz Grodzicki Katedra Chorób Wewnętrznych i Gerontologii CMUJ

2
Kardiologia geriatryczna
Nadciśnienie tętnicze Choroba niedokrwienna serca Niewydolność serca Wady serca Migotanie przedsionków

3
Nadciśnienie tętnicze w Stanach Zjednoczonych 1999 - 2000
Hypertension 2004;44:

4
Wg Avolio

5
Ryzyko udaru w zależności od wieku i SBP
Stroke mortality rate in each decade vs usual SBP at the start of that decade 120 140 160 180 Usual SBP (mm Hg) 1 2 4 8 16 32 64 128 256 Stroke mortality (floating absolute risk and 95% CI) Age at risk 80-89 years 70-79 60-69 50-59 [Lancet 2002; 360: ]
 Stroke. mortality. (floating. absolute. risk and. 95% CI) Age at risk years [Lancet 2002; 360: ]")
6
Efekty terapii nadciśnienia w wieku podeszłym

7
Diuretyk vs Ca-bloker vs ACEI – jako leki I rzutu (ALLHAT)
6.3*# 5.4 5.6 Udary 11.4 11.3 11.5 CHD (na 100 osób) 136*/ 75 135*/ 75 134/75 RR końc. 146/84 RR wyjśc. 66.9 (57.3) 66.9 (57.5) 66.9 (57.6) Śr.wiek (% >65r.ż.) ACEI Ca-bloker diuretyk * p<0.05, # u osób rasy czarnej JAMA 2002;288:
 136*/ */ /75. RR końc. 146/84. RR wyjśc (57.3) 66.9 (57.5) 66.9 (57.6) Śr.wiek (% >65r.ż.) ACEI. Ca-bloker. diuretyk. * p<0.05, # u osób rasy czarnej. JAMA 2002;288:")
8
ACEI vs diuretyk w terapii nadcisnienia w wieku podeszłym
(ANBP-2) NEJM 2003; 148.
 NEJM 2003; 148.")
9
Udary a nocny spadek ciśnienia
575 Japończyków w wieku podeszłym rezonans magnetyczny ABPM extr.dip > 20% spadek dip 10-20% nondip 0-10% reverse dip <0 % Udar zakończony zgonem- czarny Kario Hypertension 2001;38:852-7

10
Lacunar Stroke

11
Zawał w obrębie tętnicy środkowej mózgu - TK

12
Ryzyko uszkodzenia mózgu przy szybkim obniżeniu ciśnienia
Autoregulacja krążenia mózgowego przesunięta na wyższy poziom ciśnienia norma - przepływ stały przy MAP mmHg nadciśnienie - przepływ stały przy MAP mmHg Ryzyko uszkodzenia mózgu przy szybkim obniżeniu ciśnienia Nadciśnienie w wieku podeszłym dwuetapowa normalizacja ciśnienia I etap - ciśnienie < 160/90 mmHg II etap - ciśnienie < 140/90 mmHg

13
Ciśnienie tętnicze a śmiertelność całkowita w populacji > 70r. ż
Ciśnienie tętnicze a śmiertelność całkowita w populacji > 70r.ż. Krakowa Kocemba J i wsp. J Hypertens 1991;9: S286:S287

14
Osoby ciężko chore – po zawale, udarze, cukrzyca, npl, Osoby zdrowe
J Hypertens 2003; 21:49-56 Osoby ciężko chore – po zawale, udarze, cukrzyca, npl, Osoby zdrowe

15
Udary a nocny spadek ciśnienia
575 Japończyków w wieku podeszłym rezonans magnetyczny ABPM extr.dip > 20% spadek dip 10-20% nondip 0-10% reverse dip <0 % Udar zakończony zgonem- czarny Kario Hypertension 2001;38:852-7

16
The British Hypertension Society Recommendations 2004
Younger (<55 yr) and Non-Black Older (55yr) or Black Step 1 A (or B*) C or D Step 2 A (or B*) + C or D Step 3 A (or B*) + C + D Step 4 Resistant Hypertension Add: either -blocker or spironolactone or other diuretic A: ACE Inhibitor or angiotensin receptor blocker B: b - blocker C: Calcium Channel Blocker D: Diuretic (thiazide) * Combination therapy involving B and D may induce more new onset diabetes compared with other combination therapies
 and Non-Black. Older (55yr) or Black. Step 1. A (or B*) C or D. Step 2. A (or B*) + C or D. Step 3. A (or B*) + C. + D. Step 4 Resistant Hypertension. Add: either -blocker or spironolactone or other diuretic. A: ACE Inhibitor or angiotensin receptor blocker B: b - blocker C: Calcium Channel Blocker D: Diuretic (thiazide) * Combination therapy involving B and D may induce more new onset diabetes compared with other combination therapies.")
17
HYVET - Pilot “It is possible that treatment of 1000 patients for one year may reduce stroke events by 19 (9 non fatal) but may be associated with 20 extra non stroke, deaths” Bulpit et al. J Hypertens 2003;21:
 but may be associated with 20 extra non stroke, deaths Bulpit et al. J Hypertens 2003;21:")
18
Zasady leczenia chorego na nadciśnienie tętnicze
w wieku podeszłym Stopniowe, łagodne obniżanie ciśnienia Optymalne wartości w kilkuletniej perspektywie < 140/90mmHg Małe dawki leków, diuretyki, ACEI, Ca-ant. Preferowane preparaty długodziałające Analiza interakcji lekowych ( niesterydowe p-zapalne!!) Ryzyko hipotonii ortostatycznej – konieczna ocena nie tylko na początku, ale również w trakcie leczenia Konieczna współpraca z rodziną !!
 Ryzyko hipotonii ortostatycznej – konieczna ocena. nie tylko na początku, ale również w trakcie leczenia. Konieczna współpraca z rodziną !!")
19
Sytuacje szczególne – zwężenie tętnicy szyjnej, LVH, MR

20
Kardiologia geriatryczna
Nadciśnienie tętnicze Choroba niedokrwienna serca Niewydolność serca Wady serca Migotanie przedsionków

21
Zachowawcze leczenie stabilnej postaci choroby niedokrwiennej obejmuje stosowanie:
1. Leków przeciwpłytkowych i przeciwzakrzepowych, 2. Leków przeciwdławicowych: beta - blokerów nitratów, zwłaszcza o przedłużonym działaniu blokerów kanału wapniowego, leków cytoprotekcyjnych 3. Inhibitorów enzymu konwertującego, 4. Leków hipolipemizujących,

22
ACE inhibitory w CAD Poprawa funkcji rozkurczowej LK, masy LK, hamują przebudowę, śmiertelności po zawale i ryzyka ponownego zawału Stosować szczególnie u chorych po zawale ściany przedniej, z niewydolnością serca, EF < 40%, EUROPA – stabilna IHD Hipotonia, kontrola czynności nerek, stężenia potasu

23
HOPE: Pre-specified Subgroups
No. of Pts. 4169 5128 6817 2480 4355 4942 7475 1822 Placebo Rate 14.1 20.7 18.7 14.8 19.4 16.3 18.5 14.2 Age < 65 Age > 65 Male Female HTN No HTN CAD No CAD Analysis of pre-specified subgroups in the HOPE trial showed that the benefical effects of ramipril were at least as great in patients over 65 years of age as in younger patients. In addition, ramipril was associated with significant benefits in men and women, patients with or without CAD, and in patients with or without hypertension. Based on these findings, ACE inhibitor therapy should be strongly considered in all older persons with known vascular disease or diabetes.

24
Pierwotny punkt końcowy
% Śmiertelność S-N, MI lub zatrzymanie krążenia Lata 2 4 6 8 10 12 14 1 3 5 Placebo Peryndopryl p = RRR: 20% Roczna częstość zdarzeń w grupie placebo: 2.4%

25
REDUKCJA RYZYKA WYSTĄPIENIA GŁÓWNEGO PUNKTU KOŃCOWEGO
EUROPA PEACE 14 30 12 Placebo 25 Placebo 10 20 8 Zgon S-N, MI, zatrzym.krąż. Trandolapryl Zgon S-N, MI, CABG, PCI 15 6 Peryndopryl RRR = 4% p = 0,43 4 RRR = 20% p = 0,0003 10 2 5 1 2 3 4 5 1 2 3 4 5 6 Lata Lata The EUROPA Trial Investigators (the EUROPA study). Lancet 2003;362:782-8 The PEACE Trial Investigators. N Engl J Med. 2004;351:
. Lancet 2003;362: The PEACE Trial Investigators. N Engl J Med. 2004;351:")
26
Statyny w chorobie niedokrwiennej serca
Relative Risk Events Prevented Placebo Active 4S < 65 26.4% 18.1% 0.66 83 > 65 33.4% 23.6% 98 CARE 25.6% 21.1% 0.81 45 28.1% 19.7% 0.68 84 LIPID 13.4% 10.4% 0.77 30 15.5% 0.79 42 Although none of the early studies of lipid therapy enrolled elderly subjects, several of the HMG-CoA reductase inhibitor (“statin”) trials included patients up to the age of 75 years. In each of these trials, statins were well-tolerated in the elderly, relative risk reductions were similar in younger and older patients, and absolute risk reductions were greater among older patients. 4S = Scandinavian Simvastatin Survival Study; CARE = Cholesterol and Recurrent Events; LIPID = Long-term Intervention with Pravastatin in Ischemic Disease. Events Prevented refers to the number of fewer major coronary events per 1000 patients treated.
 trials included patients up to the age of 75 years. In each of these trials, statins were well-tolerated in the elderly, relative risk reductions were similar in younger and older patients, and absolute risk reductions were greater among older patients. 4S = Scandinavian Simvastatin Survival Study; CARE = Cholesterol and Recurrent Events; LIPID = Long-term Intervention with Pravastatin in Ischemic Disease. Events Prevented refers to the number of fewer major coronary events per 1000 patients treated.")
27
Effect of Simvastatin on Major Vascular Events: Heart Protection Study
Age, Years Placebo Simva-statin Events/ 1000 Pts < 65 22.1% 16.9% 51 65-69 27.2% 20.9% 63 > 70 28.7% 23.6% The Heart Protection Study randomized 20,536 patients years of age with vascular disease or diabetes to simvastatin 40 mg once daily or placebo. During a 5-year follow-up period, all-cause mortality was reduced from 14.7% in placebo-treated patients to 12.9% in simvastatin-treated patients (p=0.0003), and the proportion of patients experiencing a major vascular event was reduced by 24% with simvastatin (p<0.0001). As shown in the Table, the benefits of simvastatin therapy were evident in patients of all ages, and the number of events prevented per 1000 treated subjects was similar in older and younger patients. Source: Lancet 2002;360:7-22
, and the proportion of patients experiencing a major vascular event was reduced by 24% with simvastatin (p<0.0001). As shown in the Table, the benefits of simvastatin therapy were evident in patients of all ages, and the number of events prevented per 1000 treated subjects was similar in older and younger patients. Source: Lancet 2002;360:7-22.")
28
Znamiennie wydłuża czas do obniżenia odcinka ST o 1 mm
TRIMPOL 2 Trimetazydyna dodana do terapii ß-blokerem Znamiennie wydłuża czas do obniżenia odcinka ST o 1 mm p < 0,01 s 427,3 450 NS 381,2 metoprolol + placebo 400 357,3 metoprolol + trimetazydyna 3 x dz. 340,9 350 T0 T12 Szwed H, Sadowski Z. Eur Heart J 2001; 22:

29
European Heart Journal Cristiana Vitale 2004; 6: 1-8
Ocena działania trimetazydyny na funkcję lewej komory serca u starszych pacjentów z chorobą niedokrwienną serca i upośledzoną funkcją lewej komory (EF<50%). Próba randomizowana, podwójnie ślepa, 6 miesięczna, kontrolowana placebo; Leki (%) ACE I / sartan 100 diuretyki 96 B-blokery 72 Ca antagoniści 34 statyny 87 insulina 26 Wiek 78 po MI (%) 55 po PTCA (%) 38 po CABG (%) 30 European Heart Journal Cristiana Vitale 2004; 6: 1-8
. Próba randomizowana, podwójnie ślepa, 6 miesięczna, kontrolowana placebo; Leki (%) ACE I / sartan 100. diuretyki 96. B-blokery 72. Ca antagoniści 34. statyny 87. insulina 26. Wiek 78 po MI (%) 55 po PTCA (%) 38 po CABG (%) 30. European Heart Journal Cristiana Vitale 2004; 6: 1-8.")
30
Poprawa komfortu życia
LICZBA EPIZODÓW BÓLOWYCH / TYDZ. Liczba/tydz. p < 0,01 NS placebo 4,5 4 Trimetazydyna 3,5 3 2,5 2 1,5 1 0,5 M0 M6 M0 M6 European Heart Journal Cristiana Vitale 2004; 6: 1-8

31
European Heart Journal Cristiana Vitale 2004; 6: 1-8
Poprawa jakości życia JAKOŚĆ ŻYCIA QoL NS p < 0,01 placebo 7 6 Trimetazydyna 5 4 3 2 1 M0 M6 M0 M6 European Heart Journal Cristiana Vitale 2004; 6: 1-8

32
Angioplastyka u chorych w podeszłym wieku z dusznicą bolesną
- Niższa skuteczność 79 – 94% vs % większa częstość zmian złożonych i zwapniałych stan ogólny schorzenia towarzyszące Wyższa śmiertelność 0,8 – 11% (<70r.ż. <1%) wiek, cukrzyca, niewydolność serca EF<35%, dusznica niestabilna Większa częstość innych powikłań angioplastyki: (2 x ) zawał serca, konieczność CABG, udar mózgu, powikłania z miejsca wkłucia Główne ograniczenie - restenoza
 wiek, cukrzyca, niewydolność serca EF<35%, dusznica niestabilna. Większa częstość innych powikłań angioplastyki: (2 x ) zawał serca, konieczność CABG, udar mózgu, powikłania z miejsca wkłucia. Główne ograniczenie - restenoza.")
33
Angioplastyka u chorych w podeszłym wieku z dusznicą bolesną
W ostatnich latach poprawa rokowania: Batchelor i wsp. J.Am.Coll.Cardiol. 2000, 36 – 4 lata ryzyka zgonu o 29% ryzyka innych powikłań o 37% Mc Grath i wsp. J.Am.Coll.Cardiol. 1999,34. – 7 lat skuteczności PTCA z 88 do 93% konieczności CABG z 2,3 do 1,3% śmiertelności z 1,2 do 1,1% Ryzyko w młodszych grupach nie uległo zmianie

34
STRATEGIA PTCA W PODESZŁYM WIEKU
(choroba wielonaczyniowa) 1. Ograniczona rewaskularyzacja – poszerzenie najbardziej istotnego zwężenia: krótszy czas zabiegu, ograniczone ryzyko nagłego zamknięcia tętnicy odległe rokowanie gorsze. 2. Pełna rewaskularyzacja nie zawsze możliwa (37 – 77% vs 85% u młodych), większe ryzyko bezpośrednie, lepsze wyniki odległe.
 1. Ograniczona rewaskularyzacja – poszerzenie najbardziej istotnego zwężenia: krótszy czas zabiegu, ograniczone ryzyko nagłego zamknięcia tętnicy. odległe rokowanie gorsze. 2. Pełna rewaskularyzacja. nie zawsze możliwa (37 – 77% vs 85% u młodych), większe ryzyko bezpośrednie, lepsze wyniki odległe.")
35
Zawał serca - Fibrynoliza w podeszłym wieku
GUSTO-1 (White HD i wsp. Circulation 1996, 94) 30-dniowa śmiertelność u leczonych fibrynolitycznie wzrasta proporcjonalnie do wieku < 65 r.ż. – 3% 65 – 74 l. – 9,5% 75 – 84 l. - 19,6% > 84 r.ż. – 30,3% W obserwacji 1-rocznej większość analiz wykazała korzyść z leczenia fibrynolitycznego, ale istotnie mniejszą niż w młodszych grupach wiekowych. (Wg AHA/ACC zalecenie typu 2A; niejednoznaczne, w większości korzystne)
 30-dniowa śmiertelność u leczonych fibrynolitycznie wzrasta proporcjonalnie do wieku. < 65 r.ż. – 3% 65 – 74 l. – 9,5% 75 – 84 l. - 19,6% > 84 r.ż. – 30,3% W obserwacji 1-rocznej większość analiz wykazała korzyść z leczenia fibrynolitycznego, ale istotnie mniejszą niż w młodszych grupach wiekowych. (Wg AHA/ACC zalecenie typu 2A; niejednoznaczne, w większości korzystne)")
36
Circulation 2000, 101, 2239 – 2246 Thiemann D.R. i wsp.:
O ile w grupie chorych 65 – 75 l. tromboliza zwiększa przeżycie, dla chorych > 75 r.ż. obserwowano 30-dniowej śmiertelności, wskaźnik ryzyka – 1,38 (38% względnego ryzyka 30-dniowej śmiertelności). Zawał >75 r.ż. = 1/3 zawałów Wiek nie decyduje o wyniku fibrynolizy, ale współistniejące choroby
. Zawał >75 r.ż. = 1/3 zawałów. Wiek nie decyduje o wyniku fibrynolizy, ale współistniejące choroby.")
37
Angioplastyka vs fibrynoliza w zawale serca w podeszłym wieku
Boer i wsp. (J.Am.Coll.Cardiol. 2002,39), chorzy >75 r.ż. fibrynoliza PTCA Śmiertelność 30dn. 20% 7% Zgon+udar+zawał 29% 9% Po 1 roku 44% 13% MITRA +MIR (Zahn i wsp. J.Am.Coll.Cardiol. 2001,37) Śmiertelność w grupach wiekowych 65 – 74 l 13,4% 8,6% 75 – 84 l. 22,6% 15,4% >84 l % 5%
, chorzy >75 r.ż. fibrynoliza PTCA. Śmiertelność 30dn. 20% 7% Zgon+udar+zawał 29% 9% Po 1 roku 44% 13% MITRA +MIR (Zahn i wsp. J.Am.Coll.Cardiol. 2001,37) Śmiertelność w grupach wiekowych. 65 – 74 l 13,4% 8,6% 75 – 84 l. 22,6% 15,4% >84 l. 34% 5%")
38
Angioplastyka w zawale serca w podeszłym wieku
Odległe wyniki PTCA u osób > 70 r.ż. są lepsze niż leczenia fibrynolitycznego: Przeżycie 4-letnie – 74,8% w grupie PTCA lub CABG w zawale serca vs 49,7% w grupie nie leczonych interwencyjnie Nicolau JC i wsp.Congress of Esc Berlin 2002. Ale ryzyko PTCA wzrasta z wiekiem !

39
Angioplastyka w zawale serca w podeszłym wieku
Sakai i wsp. (Am.J.Cardiol. 2002,89) <75 r.ż. >75 r.ż. Śmiertelność wewnątrzszpitalna 3,7% 8,4% Skuteczność reperfuzji 95% 93% Śmiertelność po skutecznej 3% 6,6% Śmiertelność po nieskutecznej 18% 33% Mayo Clinic (Singh M.i wsp. Am.J.Med. 2000,108) Śmiertelność wewnątrzszpitalna: 50 – 59 lat 4% 60 – 69 lat 9% 70 – 79 lat 13% >80 lat 21%
 <75 r.ż. >75 r.ż. Śmiertelność wewnątrzszpitalna 3,7% 8,4% Skuteczność reperfuzji 95% 93% Śmiertelność po skutecznej 3% 6,6% Śmiertelność po nieskutecznej 18% 33% Mayo Clinic (Singh M.i wsp. Am.J.Med. 2000,108) Śmiertelność wewnątrzszpitalna: 50 – 59 lat 4% 60 – 69 lat 9% 70 – 79 lat 13% >80 lat 21%")
40
Leczenie zachowawcze czy inwazyjne ?
Trial of Invasive versus Medical therapy in Elderly patients with chronic symptomatic CAD: TIME. Lancet 2001; 358:951-7. 305 chorych > 75 r.ż. Z CAD leczonych inwazyjnie lub zachowawczo In the TIME study, 305 patients > 75 years of age with chronic angina despite at least 2 anti-anginal drugs were randomized to coronary angiography and revascularization or optimization of medical therapy. After 6 months follow-up, angina severity and quality of life improved to a greater extent among patients assigned to the invasive strategy. In addition, major adverse cardiac events (MACE) occurred in 49% of the patients in the medical group compared to 19% of the patients in the revascularization group (p<0.0001). This difference was related to a reduction in hospital admissions for treatment of recurrent angina, and there was no difference between groups with respect to mortality or nonfatal myocardial infarction. Indeed, there were 13 deaths in the invasive group compared to only 6 in the medical therapy group (p=0.15). Nonetheless, the findings of TIME provide further support for undertaking revascularization in selected elderly patients with symptomatic CHD.
 occurred in 49% of the patients in the medical group compared to 19% of the patients in the revascularization group (p<0.0001). This difference was related to a reduction in hospital admissions for treatment of recurrent angina, and there was no difference between groups with respect to mortality or nonfatal myocardial infarction. Indeed, there were 13 deaths in the invasive group compared to only 6 in the medical therapy group (p=0.15). Nonetheless, the findings of TIME provide further support for undertaking revascularization in selected elderly patients with symptomatic CHD.")
41
Kardiologia geriatryczna
Nadciśnienie tętnicze Choroba niedokrwienna serca Niewydolność serca Wady serca Migotanie przedsionków

42
Z NIEWYDOLNOŚCIĄ SERCA
ŚREDNIA WIEKU CHORYCH Z NIEWYDOLNOŚCIĄ SERCA 80 70 60 50 40 Wiek (lata) 30 20 10 Rosja Polska Węgry Szwecja Niemcy Belgia Turcja Holandia Francja Włochy Szwajcaria Hiszpania Czechy / Słowacja Wielka Brytania IMPROVEMENT 2000
 Rosja. Polska. Węgry. Szwecja. Niemcy. Belgia. Turcja. Holandia. Francja. Włochy. Szwajcaria. Hiszpania. Czechy / Słowacja. Wielka Brytania. IMPROVEMENT")
43
Wiek pacjentów leczonych w Polsce z powodu NS – badanie POLKARD 2005 /lecznictwo otwarte/
Losowa próba 400 lekarzy rodzinnych – 2000 pacjentów

44
Wiek pacjentów hospitalizowanych z powodu NS we Francji
200 n 150 100 A survey study conducted in all patients hospitalised in France for heart failure, showed that their mean age was >75 years, about15 years more than the mean age of patients entered in major clinical trials. 50 Wiek (lata) 27-40 40-50 50-60 60-65 65-70 70-75 75-80 80-85 85-90 90-95 90-95 Cohen Solal A, Eur Heart J 2000
 Cohen Solal A, Eur Heart J")
45
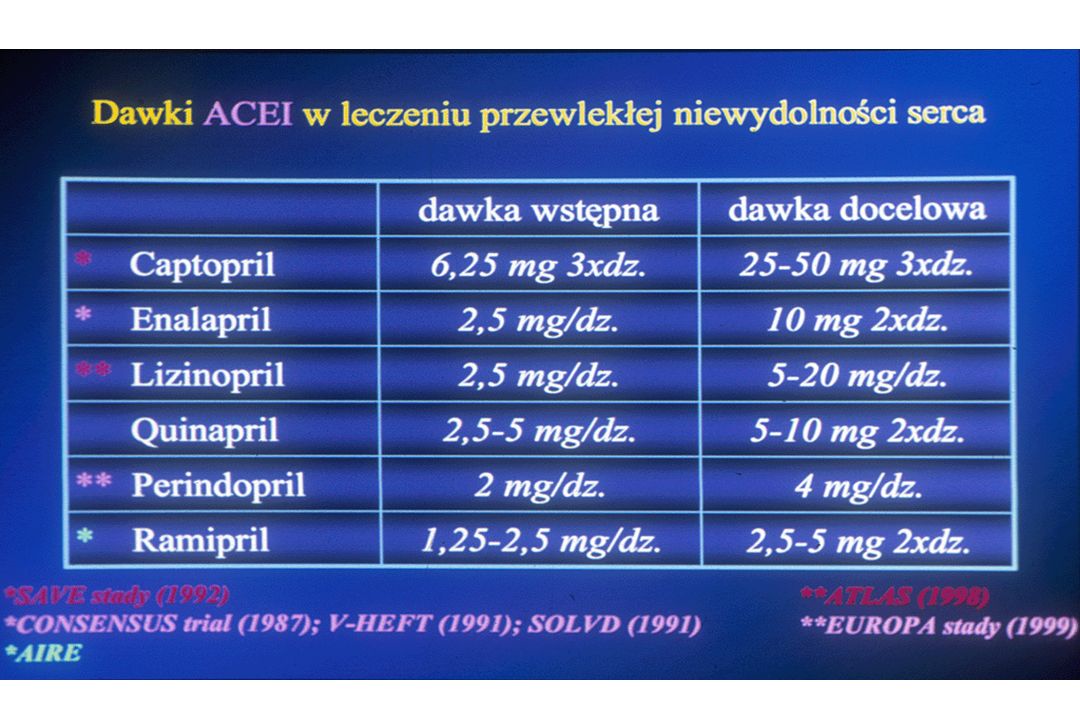
Leczenie farmakologiczne
Niewydolność serca Leczenie farmakologiczne Inhibitory konwertazy angiotensyny ß-blokery Diuretyki Spironolakton Glikozydy naparstnicy Nitraty / Hydralazyna

46
STOSOWANIE INHIBITORÓW ACE
I BETA BLOKERÓW % poniżej 70 r.ż. 70 r.ż. i powyżej 100 90 80 70 60 50 40 30 20 10 Rosja Polska Węgry Szwecja Niemcy Belgia Holandia Francja Włochy Turcja Szwajcaria Hiszpania Wielka Brytania Czechy / Słowacja

47
STOSOWANIE BETA - BLOKERÓW
poniżej 70 r.ż. 70 r.ż. i powyżej % 100 90 80 70 60 50 40 30 20 10 Rosja Polska Węgry Szwecja Niemcy Belgia Holandia Francja Włochy Turcja Szwajcaria Hiszpania Czechy / Słowacja Wielka Brytania

48
Wysoka śmiertelność >20% Bez upośledzonej funkcji lewej komory
Niska śmiertelność <20% <10% 0% Wysokie ryzyko CVE Niskie ryzyko CVE 100% Niska EF CONSENSUS I Populacja z chorobą wieńcową SOLVDt Niewydolność krążenia jawna klinicznie SAVE AIRE TRACE 35% Bez klinicznych cech niewydolności krążenia SOLVDp 35- 40% HOPE Bez upośledzonej funkcji lewej komory EUROPA Prawidłowa EF S.Grajek 2003

49
Wiek pacjentów z NS w głównych programach z ß-Blokerami
Średni wiek BEST Bucindolol 2708 60 CIBIS-I Bisoprolol 641 60 CIBIS-II Bisoprolol 2647 61 COPERNICUS Carvedilol 2289 63 MERIT-HF Metoprolol CR/XL 3991 64 The average age of patients in these previous studies of beta-blockers in heart failure has been 63 years which is not representative of the real population. US Carvedilol Carvedilol 1094 58 COMET Carvedilol / Metoprolol CR 3029 62

50
SENIORS SENIORS Study of Effects of Nebivolol Intervention on Outcomes and Rehospitalisation in Seniors with Heart Failure The SENIORS study was performed to assess the effects of the highly selective beta-blocker nebivolol in patients > 70 years, regardless of ejection fraction. In large randomized trials it was shown that in patients with heart failure treated with beta-blockers, mortality and hospital admissions were reduced, but the effect of betablockers in elderly patients with a broad range of LVEF are uncertain.

51
Baseline Characteristics
Nebivolol Placebo Age (mean, yrs) 76.1 76.1 Male (n, %) 657 (61.6) 686 (64.7) LVEF 35 % (n, %) * 683 (64.3) 686 (64.8) LVEF (mean, %) 36.0 36.0 NYHA Class (n, %) I 32 (3.0) 29 (2.7) II 603 (56.5) 597 (56.3) SENIORS patients mean age almost exactly reflects the mean age of heart failure patients in the community, being over 76 years old. Moreover,it included the important group of patients with preserved sysotolic function (more than one-third of these patients had heart failure with left ventricular ejection fraction > 35%) III 413 (38.7) 411 (38.7) IV 19 (1.8) 24 (2.3) * 7 patients with missing LVEF at baseline
 Male (n, %) 657 (61.6) 686 (64.7) LVEF 35 % (n, %) * 683 (64.3) 686 (64.8) LVEF (mean, %) NYHA Class (n, %) I. 32 (3.0) 29 (2.7) II. 603 (56.5) 597 (56.3) SENIORS patients mean age almost exactly reflects the mean age of heart failure patients in the community, being over 76 years old. Moreover,it included the important group of patients with preserved sysotolic function (more than one-third of these patients had heart failure with left ventricular ejection fraction > 35%) III. 413 (38.7) 411 (38.7) IV. 19 (1.8) 24 (2.3) * 7 patients with missing LVEF at baseline.")
52
All Cause Mortality or CV Hospital Admission (Primary Outcome)
No. of events: Nebivolol 332 (31.1%) Placebo 375 (35.3%) Event free Survival % Hazard Ratio 0.86 [0.74;0.99] p = 0.039 There was a statistically significant reduction in the primary outcome of 14% and that reflects, given the high event rate in older patients, a substantial reduction in events. There were 43 fewer events in the nebivolol group than in the placebo group, which is equivalent to an absolute reduction of 4.2%. Of those 43 patients who had a major event prevented, there were 23 prevented deaths and 20 prevented cardiovascular hospital admissions Those events were evenly distributed between reductions in mortality and reductions in cardiovascular hospital admissions.
 Placebo 375 (35.3%) Event free. Survival % Hazard Ratio 0.86 [0.74;0.99] p = There was a statistically significant reduction in the primary outcome of 14% and that reflects, given the high event rate in older patients, a substantial reduction in events. There were 43 fewer events in the nebivolol group than in the placebo group, which is equivalent to an absolute reduction of 4.2%. Of those 43 patients who had a major event prevented, there were 23 prevented deaths and 20 prevented cardiovascular hospital admissions Those events were evenly distributed between reductions in mortality and reductions in cardiovascular hospital admissions.")
53
Secondary Endpoint – Cardiovascular mortality or cardiovascular hospital admission
Event free Survival % 100% Nebivolol Placebo 90% Hazard Ratio 0.84 [0.72;0.98] p = 0.027 80% 70% 60% Moreover, the combined end point of cardiovascular mortality or cardiovascular hospital admission (time to first event), was significantly reduced by 16% 50% 40% 3 6 9 12 15 18 21 24 27 30 33 36 39 Time (months) Number of events: Nebivolol 305 (28.6%) Placebo (33.3%)
, was significantly reduced by 16% 50% 40% Time (months) Number of events: Nebivolol 305 (28.6%) Placebo 350 (33.3%)")
54
Death or CV Hospitalisation by Subgroup
Nebivolol Placebo Favours Nebivolol Favours Placebo 125 (33.6%) 110 (28.9%) > 35 % LVEF 249 (36.3%) 219 (32.1%) 35 % 125 (33.3%) 101 (24.6%) Female Sex 250 (36.4%) 231 (35.2%) Male 199 (37.1%) 184 (34.8%) > 75 y Age 176 (33.5%) 148 (27.5%) 70-75 y There is no statistically significant interactions between the subgroups and the outcome. Concerning the ejection fraction the results are similar; the group of patients with an ejection fraction above 35% had a greater point estimate for protection in this study. There is absolute reassurance that elderly female patients with heart failure definitively benefit from the introduction of nebivolol as a recommended beta-blocker. There was an individually significant result for over 1,000 patients aged between years old 375 (35.3%) 332 (31.1%) Total Hazard ratio and 95% CI 0.50 0.60 0.70 0.80 0.90 1.00 1.10 1.20
 110 (28.9%) > 35 % LVEF. 249 (36.3%) 219 (32.1%) 35 % 125 (33.3%) 101 (24.6%) Female. Sex. 250 (36.4%) 231 (35.2%) Male. 199 (37.1%) 184 (34.8%) > 75 y. Age. 176 (33.5%) 148 (27.5%) y. There is no statistically significant interactions between the subgroups and the outcome. Concerning the ejection fraction the results are similar; the group of patients with an ejection fraction above 35% had a greater point estimate for protection in this study. There is absolute reassurance that elderly female patients with heart failure definitively benefit from the introduction of nebivolol as a recommended beta-blocker. There was an individually significant result for over 1,000 patients aged between years old. 375 (35.3%) 332 (31.1%) Total. Hazard ratio and 95% CI")
55
Benefit of beta-blockers - comparison of Hazard Ratio
Favours treatment Favours placebo Primary outcome SENIORS- Overall SENIORS - Age < 75 y & LVEF < 35% MERIT-HF - Age >65 y mean age 71.8 All cause mortality SENIORS - Overall - Age < 75 y & LVEF < 35% CIBIS II (HR 0.66) MERIT HF (HR 0.66) MERIT-HF - (HR 0.63) Age >65 (m 71.8) COPERNICUS (HR 0.65) In order to put the results of SENIORS in the context of previous beta-blocker trials, which recruited younger patients and excluded patients with higher ejection fractions, the subgroup of patients most similar to the previous major outcome trials was identified. In this subgroup, defined as patients less than 75 years old with an ejection fraction < 35% (n= 342 for nebivolol and n= 342 for placebo), the Hazard Ratio for the primary outcome was 0.73 (95% CI 0.56–0.96). For all cause mortality alone, the HR was 0.62 (95% CI 0.43–0.89).Moreover, a similar subgroup analysis was conducted in MERIT-HF (992 patients with age > 65, mean age 71.8).In this population, metoprolol showed a HR of 0.63 (95%CI ) in total mortality and 0.70 (95%CI ) in the combined all cause mortality and hospitalization due to worsening heart failure. This suggests for nebivolol an efficacy comparable to that demonstrated by other beta blockers in previous clinical trials. * 0.40 0.50 0.60 0.70 0.80 0.90 1.00 1.10 1.20 Hazard ratio and 95% CI
 MERIT HF (HR 0.66) MERIT-HF - (HR 0.63) Age >65 (m 71.8) COPERNICUS (HR 0.65) In order to put the results of SENIORS in the context of previous beta-blocker trials, which recruited younger patients and excluded patients with higher ejection fractions, the subgroup of patients most similar to the previous major outcome trials was identified. In this subgroup, defined as patients less than 75 years old with an ejection fraction < 35% (n= 342 for nebivolol and n= 342 for placebo), the Hazard Ratio for the primary outcome was 0.73 (95% CI 0.56–0.96). For all cause mortality alone, the HR was 0.62 (95% CI 0.43–0.89).Moreover, a similar subgroup analysis was conducted in MERIT-HF (992 patients with age > 65, mean age 71.8).In this population, metoprolol showed a HR of 0.63 (95%CI ) in total mortality and 0.70 (95%CI ) in the combined all cause mortality and hospitalization due to worsening heart failure. This suggests for nebivolol an efficacy comparable to that demonstrated by other beta blockers in previous clinical trials. * Hazard ratio and 95% CI.")
57
Dawki beta-adrenolityków w NS w wieku podeszłym
Lek Dawka początkowa Dawka optymalna Karwedilol 3,125 mg – zwiększanie ok. 6 tyg. 50 mg Bisoprolol 1,25 mg – zwiększanie ok.12 tyg. 10 mg Metoprolol 5 mg – zwiększanie ok. 6 tyg. / 200 Metoprolol CR Nebivolol 1,25 mg – zwiększanie ok tyg. 10 mg

58
Readmission Rates Within 90 Days in Elderly Patients
First Admission Vinson JM, et al., J Am Geriatr Soc, 1990;38:1290

59
Kaplan-Meier Curves for the Probability of Not Being Readmitted to the Hospital during the 90-Day Period of Follow-up Figure 1. Kaplan-Meier Curves for the Probability of Not Being Readmitted to the Hospital during the 90-Day Period of Follow-up. Data on patients who died without being readmitted were censored at the time of death. Rich, M. W. et al. N Engl J Med 1995;333:

60
Intensywna edukacja na temat istoty NS i leczenia.
Interwencja: Intensywna edukacja na temat istoty NS i leczenia. Indywidualne porady dietetyczne. Kontakt z pracownikami socjalnymi i lekarzem rodzinnym. Konsultacje leczenia z geriatrą w celu eliminacji zbędnych leków. Intensywna opieka poszpitalna – kontakt z rodziną, telefoniczne kontrole. Koszty (na pacjenta): Kontrola Interwencja Interwencja Opiekunowie Inne koszty medyczne Re-hospitalizacje Wszystkie: $ Rich, M. W. et al. N Engl J Med 1995;333:
: Kontrola Interwencja. Interwencja Opiekunowie Inne koszty medyczne Re-hospitalizacje Wszystkie: $ Rich, M. W. et al. N Engl J Med 1995;333:")
61
Schorzenia współistniejące u chorych z NS w zależności do wieku
Schorzenie Wszyscy Młodsi Starsi >65 r.ż. M.Fedyk-Łukasik 2005

62
NIEWYDOLNOŚCI SERCA Definicja Skurczowa Rozkurczowa 1 + EF ≥ 45%
+ cechy nieprawidłowej relaksacji, rozkurczowej rozciągliwości lub sztywności 1 + EF < 45% + 3 zwolnienie szybkości skracania sarkomerów (kurczliwość) upośledzenie czynności serca jako pompy spadek „rzutu” serca ograniczenie przepływu tkankowego utrudniony lub częściowy powrót miofibrylli do długości spoczynkowej niskie ciśnienie napełniania upośledza czynność LK napełnianie LK jest wolne i niepełne do chwili skurczu przedsionka POBUDZENIE UKŁADÓW NEUROHUMORALNYCH NIEPRAWIDŁOWA CZYNNOŚĆ NEREK POBUDZENIE UKŁADÓW NEUROHUMORALNYCH (?) chyba że wtórnie do przestrojenia baroreceptorów NIEPRAWIDŁOWA CZYNNOŚĆ NEREK (?) (ESC, Braunwald, Poole-Wilson Gaasch) (Gaasch, Zile 2004) Korewicki J 2005
 upośledzenie czynności serca jako pompy. spadek „rzutu serca. ograniczenie przepływu tkankowego. utrudniony lub częściowy powrót miofibrylli. do długości spoczynkowej. niskie ciśnienie napełniania upośledza. czynność LK. napełnianie LK jest wolne i niepełne do chwili. skurczu przedsionka. POBUDZENIE UKŁADÓW NEUROHUMORALNYCH. NIEPRAWIDŁOWA CZYNNOŚĆ NEREK. POBUDZENIE UKŁADÓW NEUROHUMORALNYCH ( ) chyba że wtórnie do przestrojenia baroreceptorów. NIEPRAWIDŁOWA CZYNNOŚĆ NEREK ( ) (ESC, Braunwald, Poole-Wilson. Gaasch) (Gaasch, Zile 2004) Korewicki J")
63
POSTĘPOWANIE Z CHORYMI Z NIEWYDOLNOŚCIĄ SERCA
Skurczowa Rozkurczowa ustalenie etiologii leczenie przyczynowe modyfikacje przebudowy serca kontrola wolemii utrzymanie rytmu zatokowego ustalenie etiologii leczenie przyczynowe kontrola wolemii utrzymanie rytmu zatokowego modyfikacja przebudowy serca (?) leczenie farmakologiczne leczenie farmakologiczne ACE.I lub/i ARB beta blokery diuretyki naparstnica antagoniści aldosteronu diuretyki nitraty beta blokery blokery kanałów wapniowych blokery ARB lub ACE.I UZNANE STANDARDY LECZENIA liczne wieloośrodkowe randomizowane badania lekowe (poziom wiarygodności A) BRAK STANDARDÓW LECZENIA pojedyncze, randomizowane badania lekowe (poziom wiarygodności C) Korewicki J 2005
 leczenie farmakologiczne. leczenie farmakologiczne. ACE.I lub/i ARB. beta blokery. diuretyki. naparstnica. antagoniści aldosteronu. diuretyki. nitraty. beta blokery. blokery kanałów wapniowych. blokery ARB lub ACE.I. UZNANE STANDARDY LECZENIA. liczne wieloośrodkowe randomizowane. badania lekowe (poziom wiarygodności A) BRAK STANDARDÓW LECZENIA. pojedyncze, randomizowane badania. lekowe (poziom wiarygodności C) Korewicki J")
64
Kardiologia geriatryczna
Nadciśnienie tętnicze Choroba niedokrwienna serca Niewydolność serca Wady serca Migotanie przedsionków

65
Luc A. Pierard, M.D., Ph.D. and Patrizio Lancellotti, M.D.
The Role of Ischemic Mitral Regurgitation in the Pathogenesis of Acute Pulmonary Edema Luc A. Pierard, M.D., Ph.D. and Patrizio Lancellotti, M.D. N Engl J Med Volume 351;16: October 14, 2004

66
Mid-Systolic Apical Four-Chamber View Obtained at Rest and during Exercise in a Patient Who Presented with Acute Pulmonary Edema Pierard, L. et al. N Engl J Med 2004;351:

67
Study Overview In patients with ischemic heart disease, mitral regurgitation may be a dynamic phenomenon, increasing or decreasing on the basis of changes in loading conditions or left ventricular geometry This study shows that transient increases in the severity of mitral regurgitation may have an important role in the pathogenesis of acute pulmonary edema Interventions to reduce or prevent mitral regurgitation might be beneficial

68
Base-Line Characteristics of the Subjects with Normal Aortic Valves, Those with Sclerotic Valves, and Those with Stenotic Valves Table 1. Base-Line Characteristics of the Subjects with Normal Aortic Valves, Those with Sclerotic Valves, and Those with Stenotic Valves. Otto, C. M. et al. N Engl J Med 1999;341:

69
Event Rates in the Three Groups
Table 2. Event Rates in the Three Groups. Otto, C. M. et al. N Engl J Med 1999;341:

70
Rates and Relative Risks of Death from Any Cause and of Death from Cardiovascular Causes among the 4073 Subjects with No Coronary Heart Disease at Entry, According to the Presence or Absence of Aortic Sclerosis Table 3. Rates and Relative Risks of Death from Any Cause and of Death from Cardiovascular Causes among the 4073 Subjects with No Coronary Heart Disease at Entry, According to the Presence or Absence of Aortic Sclerosis. Otto, C. M. et al. N Engl J Med 1999;341:

71
Survival among Patients with Severe Symptomatic Aortic Stenosis Who Underwent Valve Replacement and Similar Patients Who Declined to Undergo Surgery Figure 1. Survival among Patients with Severe Symptomatic Aortic Stenosis Who Underwent Valve Replacement and Similar Patients Who Declined to Undergo Surgery. The overall and individual P values are shown, as is the overall chi-square value. Reprinted from Schwarz et al.11 with the permission of the publisher. Carabello, B. A. N Engl J Med 2002;346:

72
Recommendations for the Use of Aortic-Valve Replacement in Patients with Aortic Stenosis
Table 2. Recommendations for the Use of Aortic-Valve Replacement in Patients with Aortic Stenosis. Carabello, B. A. N Engl J Med 2002;346:

73
Kardiologia geriatryczna
Nadciśnienie tętnicze Choroba niedokrwienna serca Niewydolność serca Wady serca Migotanie przedsionków

74
ATRIA: Prevalence of AF by age and sex Content Points:
The AnTicoagulation and Risk factors In Atrial fibrillation (ATRIA) study was a cross-sectional prevalence study in adults who were enrolled in a large California health maintenance organization (Kaiser Permanente of Northern California).1 In the study population of 1.89 million, a diagnosis of AF was entered in the medical records of 17,974 patients (0.95%) between July 1, 1996 and December 31, 1997. The prevalence of AF was greater in men than in women, and increased with age in both groups. 1Go AS, Hylek EM, Phillips KA, Chang Y, Henault LE, Selby JV, Singer DE. Prevalence of diagnosed atrial fibrillation in adults: National implications for rhythm management and stroke prevention: The AnTicoagulation and Risk factors In Atrial fibrillation (ATRIA) study. JAMA.2001;285:
 study was a cross-sectional prevalence study in adults who were enrolled in a large California health maintenance organization (Kaiser Permanente of Northern California).1. In the study population of 1.89 million, a diagnosis of AF was entered in the medical records of 17,974 patients (0.95%) between July 1, 1996 and December 31, The prevalence of AF was greater in men than in women, and increased with age in both groups. 1Go AS, Hylek EM, Phillips KA, Chang Y, Henault LE, Selby JV, Singer DE. Prevalence of diagnosed atrial fibrillation in adults: National implications for rhythm management and stroke prevention: The AnTicoagulation and Risk factors In Atrial fibrillation (ATRIA) study. JAMA.2001;285:")
75
ATRIA: Projected number of patients with AF Content Points:
The ATRIA investigators estimated that 2.08 million Americans had AF during the period of cohort assembly and that this would rise to 5.61 million by 2050, an increase of approximately 2.5-fold.1 This increase reflects the projected increase in elderly individuals in the US population. 1Go AS, Hylek EM, Phillips KA, Chang Y, Henault LE, Selby JV, Singer DE. Prevalence of diagnosed atrial fibrillation in adults: National implications for rhythm management and stroke prevention: The AnTicoagulation and Risk factors In Atrial fibrillation (ATRIA) study. JAMA. 2001;285:
 study. JAMA. 2001;285:")
76
Hospitalizations for AF are increasing Content Points:
Wattigney et al used data from the National Hospital Discharge Survey to study US trends in hospitalization for AF between 1985 and In this study, the investigators used ICD-9-CM diagnosis codes and to identify patients with AF. These codes include both AF and atrial flutter. Total hospitalizations for AF as the principal diagnosis increased from 154,086 to 376,487 (144% change). Hospitalizations for AF as a principal or secondary diagnosis followed a similar trend: 787,750 to 2,283,763 (190% change). As shown, while rates for individuals aged <64 years remained relatively level, the rates for individuals aged >65 years have risen. 1Wattigney WA, Mensah GA, Croft JB. Increasing trends in hospitalization for atrial fibrillation in the United States, 1985 through 1999: Implications for primary prevention. Circulation. 2003;108:
. Hospitalizations for AF as a principal or secondary diagnosis followed a similar trend: 787,750 to 2,283,763 (190% change). As shown, while rates for individuals aged <64 years remained relatively level, the rates for individuals aged >65 years have risen. 1Wattigney WA, Mensah GA, Croft JB. Increasing trends in hospitalization for atrial fibrillation in the United States, 1985 through 1999: Implications for primary prevention. Circulation. 2003;108:")
77
Mortality and AF Content Points:
Wolf et al conducted a prospective cohort study of 26,753 hospitalized patients with cardiovascular disease; 13,558 patients also had AF; 13,195 patients did not.1 The slide summarizes mortality rates by age and sex during the 3-year study period. Patients with AF had significantly higher mortality rates than matched patients without AF. 1Wolf PA, Mitchell JB, Baker CS, Kannel WB, D'Agostino RB. Impact of atrial fibrillation on mortality, stroke, and medical costs. Arch Intern Med. 1998;158:

78
A. Epidemiology update:
2. Stroke and AF Embolic stroke Content Points: Stroke accounts for much of the morbidity and mortality associated with AF.

79
Stroke risk is increased in AF Content Points:
Framingham Heart Study investigators examined the impact of AF on stroke risk in 5184 male and female participants.1 Age-specific prevalence rates increased steadily from 1.8% for ages years to 10.2% for ages years. In each age group, stroke rates were approximately 5-fold higher in groups with AF compared with groups without AF. The percent of total stroke events attributed to AF (population attributable risk) increased from 7.3% in years age group to 30.8% in the years age group. 1Wolf PA, Abbott RD, Kannel WB. Atrial fibrillation: A major contributor to stroke in the elderly. Arch Intern Med. 1987;147:
 increased from 7.3% in years age group to 30.8% in the years age group. 1Wolf PA, Abbott RD, Kannel WB. Atrial fibrillation: A major contributor to stroke in the elderly. Arch Intern Med. 1987;147:")
80
Severity of stroke with AF Content Points:
Dulli et al reviewed the clinical presentations of patients with acute ischemic stroke admitted between 1990 and Of 1061 patients with acute ischemic stroke, 216 (20.3%) had AF. The frequency of bedridden state was 41.2% in patients with AF compared with 23.7% in patients without AF (P < ). The odds ratio for bedridden state following ischemic stroke due to AF was 2.23 (95% confidence interval [CI], ; P < ) by multivariate logistic regression. The investigators concluded that ischemic stroke associated with AF is typically more severe than ischemic stroke due to other etiologies, and this increased severity is independent of advanced age and other stroke risk factors. 1Dulli DA, Stanko H, Levine RL. Atrial fibrillation is associated with severe acute ischemic stroke. Neuroepidemiology. 2003;22:
 had AF. The frequency of bedridden state was 41.2% in patients with AF compared with 23.7% in patients without AF (P < ). The odds ratio for bedridden state following ischemic stroke due to AF was 2.23 (95% confidence interval [CI], ; P < ) by multivariate logistic regression. The investigators concluded that ischemic stroke associated with AF is typically more severe than ischemic stroke due to other etiologies, and this increased severity is independent of advanced age and other stroke risk factors. 1Dulli DA, Stanko H, Levine RL. Atrial fibrillation is associated with severe acute ischemic stroke. Neuroepidemiology. 2003;22:")
81
SPAF III: Stroke/systemic embolism event rates according to TEE findings
Content Points: Transesophageal echocardiography (TEE) offers several advantages over transthoracic echocardiography (TTE) for clot visualization. It provides a clearer view of the left atrial appendage, permits measurement of left atrial appendicular flow and outflow blood velocity, enhances clot identification, and possibly improves stroke risk estimate.1 Investigators from the SPAF III trial analyzed TEE data from 42 patients to determine the correlation between specific TEE findings and embolic risk.2 As illustrated on the slide, TEE findings suggestive of left atrial abnormality or complex aortic plaque identified high-risk patients. There was a 7.8% rate of stroke or systemic emboli in patients with left atrial abnormality (thrombus, dense spontaneous echocardiographic contrast, or peak antegrade velocity of blood flow <20 cm/s). There was a 12% event rate in patients with complex aortic plaque. There was a 20.5% event rate in patients with both left atrial abnormality and complex plaque. Conversely, there was a much lower event rate (1.3%) in patients with neither left atrial abnormality or complex plaque. 1Manning WJ, Weintraub RM, Waksmonski CA, Haering JM, Rooney PS, Maslow AD, et al. Accuracy of transesophageal echocardiography for identifying left atrial thrombi: A prospective, intraoperative study. Ann Intern Med. 1995;123: SPAF Investigators Committee on Echocardiography. Transesophageal echocardiographic correlates of thrombo embolism in high-risk patients with nonvalvular atrial fibrillation. Ann Intern Med. 1998;128:
 offers several advantages over transthoracic echocardiography (TTE) for clot visualization. It provides a clearer view of the left atrial appendage, permits measurement of left atrial appendicular flow and outflow blood velocity, enhances clot identification, and possibly improves stroke risk estimate.1. Investigators from the SPAF III trial analyzed TEE data from 42 patients to determine the correlation between specific TEE findings and embolic risk.2. As illustrated on the slide, TEE findings suggestive of left atrial abnormality or complex aortic plaque identified high-risk patients. There was a 7.8% rate of stroke or systemic emboli in patients with left atrial abnormality (thrombus, dense spontaneous echocardiographic contrast, or peak antegrade velocity of blood flow <20 cm/s). There was a 12% event rate in patients with complex aortic plaque. There was a 20.5% event rate in patients with both left atrial abnormality and complex plaque. Conversely, there was a much lower event rate (1.3%) in patients with neither left atrial abnormality or complex plaque. 1Manning WJ, Weintraub RM, Waksmonski CA, Haering JM, Rooney PS, Maslow AD, et al. Accuracy of transesophageal echocardiography for identifying left atrial thrombi: A prospective, intraoperative study. Ann Intern Med. 1995;123: SPAF Investigators Committee on Echocardiography. Transesophageal echocardiographic correlates of thrombo embolism in high-risk patients with nonvalvular atrial fibrillation. Ann Intern Med. 1998;128:")
82
Potential prothrombotic mechanisms in AF: ↓ NO production
Content Points: Cai et al studied nitric oxide (NO) production in the left atrial endocardium of pigs with experimentally induced AF.1 As shown, basal NO levels were significantly lower in the left atrium and LAA in animals with AF compared with controls without AF (P < 0.01 for both comparisons). This was accompanied by a 46% decrease in expression of NO synthase (NOS) in the left atrium of animals with AF compared with controls (P < 0.01, data not shown). AF did not cause significant changes in NO levels of NOS expression in the right atria or ascending aorta. The investigators concluded that organized atrial contraction is required to maintain normal endocardial expression of NO. Since NO has important antithrombotic effects, the investigators speculate that decreased NO bioavailability may contribute to clot formation. 1Cai H, Li Z, Goette A, Mera F, Honeycutt C, Feterik K, et al. Downregulation of endocardial nitric oxide synthase expression and nitric oxide production in atrial fibrillation: Potential mechanisms for atrial thrombosis and stroke. Circulation. 2002;106:
 production in the left atrial endocardium of pigs with experimentally induced AF.1. As shown, basal NO levels were significantly lower in the left atrium and LAA in animals with AF compared with controls without AF (P < 0.01 for both comparisons). This was accompanied by a 46% decrease in expression of NO synthase (NOS) in the left atrium of animals with AF compared with controls (P < 0.01, data not shown). AF did not cause significant changes in NO levels of NOS expression in the right atria or ascending aorta. The investigators concluded that organized atrial contraction is required to maintain normal endocardial expression of NO. Since NO has important antithrombotic effects, the investigators speculate that decreased NO bioavailability may contribute to clot formation. 1Cai H, Li Z, Goette A, Mera F, Honeycutt C, Feterik K, et al. Downregulation of endocardial nitric oxide synthase expression and nitric oxide production in atrial fibrillation: Potential mechanisms for atrial thrombosis and stroke. Circulation. 2002;106:")
83
Potential prothrombotic mechanisms in AF: LAA stasis Content Points:
The Stroke Prevention in Atrial Fibrillation (SPAF) clinical trial program was sponsored by the National Institute of Neurological Disorders and Stroke and consisted of six multicenter clinical trials of antithrombotic therapy (warfarin, aspirin) in patients with AF.1 SPAF III was an evaluation of a risk stratification scheme developed from the SPAF I and II data, and compared dose-adjusted warfarin (INR 2-3) with fixed-dose, low-intensity warfarin plus aspirin in high-risk patients. There was a 74% risk reduction for dose-adjusted warfarin vs the combination anticoagulation regimen. To explore the mechanism of clot formation, investigators used TEE to assess flow velocity in the LAA in a cohort of 721 patients.2 Peak antegrade flow velocity (Avp) was used as a measure of LAA emptying. Among patients with Avp<20 cm/s, 20 to 30 cm/s, and >30 cm/s, the frequencies of LAA thrombi were 17%, 6%, and 6%, respectively. When patients treated with adjusted-dose warfarin and those with noncardioembolic stroke were excluded from the analysis, reduced Avp was shown to be predictive of cardioembolic events (as shown on the slide). In high-risk patients, the frequency of LAA thrombus and cardioembolic events increased more than 2.5-fold when Avp was <20 cm/s. These findings demonstrate that reduced LAA flow velocity is important in the genesis of clots. 1Hart RG. Lessons from the Stroke Prevention in Atrial Fibrillation trials. Ann Intern Med. 2003;138: 2Goldman ME, Pearce LA, Hart RG, Zabalgoitia M, Asinger RW, Safford R, Halperin JL, for the Stroke Prevention in Atrial Fibrillation Investigators. Pathophysiologic correlates of thromboembolism in nonvalvular atrial fibrillation: I. Reduced flow velocity in the left atrial appendage (the Stroke Prevention in Atrial Fibrillation [SPAF-III] study). J Am Soc Echocardiogr. 1999;12:
 clinical trial program was sponsored by the National Institute of Neurological Disorders and Stroke and consisted of six multicenter clinical trials of antithrombotic therapy (warfarin, aspirin) in patients with AF.1. SPAF III was an evaluation of a risk stratification scheme developed from the SPAF I and II data, and compared dose-adjusted warfarin (INR 2-3) with fixed-dose, low-intensity warfarin plus aspirin in high-risk patients. There was a 74% risk reduction for dose-adjusted warfarin vs the combination anticoagulation regimen. To explore the mechanism of clot formation, investigators used TEE to assess flow velocity in the LAA in a cohort of 721 patients.2. Peak antegrade flow velocity (Avp) was used as a measure of LAA emptying. Among patients with Avp<20 cm/s, 20 to 30 cm/s, and >30 cm/s, the frequencies of LAA thrombi were 17%, 6%, and 6%, respectively. When patients treated with adjusted-dose warfarin and those with noncardioembolic stroke were excluded from the analysis, reduced Avp was shown to be predictive of cardioembolic events (as shown on the slide). In high-risk patients, the frequency of LAA thrombus and cardioembolic events increased more than 2.5-fold when Avp was <20 cm/s. These findings demonstrate that reduced LAA flow velocity is important in the genesis of clots. 1Hart RG. Lessons from the Stroke Prevention in Atrial Fibrillation trials. Ann Intern Med. 2003;138: Goldman ME, Pearce LA, Hart RG, Zabalgoitia M, Asinger RW, Safford R, Halperin JL, for the Stroke Prevention in Atrial Fibrillation Investigators. Pathophysiologic correlates of thromboembolism in nonvalvular atrial fibrillation: I. Reduced flow velocity in the left atrial appendage (the Stroke Prevention in Atrial Fibrillation [SPAF-III] study). J Am Soc Echocardiogr. 1999;12:")
84
Stroke mechanisms in AF: Proposed unifying model Content Points:
Cardiovascular risk factors such as elevated blood pressure, coronary artery disease (CAD), and diabetes likely account in large part for the hypercoagulable state associated with AF.1 However, the observation that markers of coagulation activity increase when the duration of AF is >12 hours suggests that AF per se may contribute to enhancement of coagulation.2 The role of cardiovascular risk factors in decreased NO bioavailability in the coronary vascular endothelium is well established.3 Thus, it is reasonable to speculate that they may also contribute to the downregulation of endocardial NOS.4 However, mechanical factors secondary to disorganized atrial contraction may also play a role.4 Decreased NO bioavailability, in turn, leads to an environment conducive to platelet adhesion to the endocardium and an altered fibrinolytic balance (increased PAI-1). Since activation of the coagulation system with subsequent thrombin formation is the primary pathogenic mechanism, the result is a fibrin-rich clot. 1Feng D, D'Agostino RB, Silbershatz H, Lipinska I, Massaro J, Levy D, et al. Hemostatic state and atrial fibrillation (the Framingham Offspring Study). Am J Cardiol. 2001;87: 2Sohara H, Amitani S, Kurose M, Miyahara K. Atrial fibrillation activates platelets and coagulation in a time-dependent manner: a study in patients with paroxysmal atrial fibrillation. J Am Coll Cardiol. 1997;29: 3Cai H, Harrison DG. Endothelial dysfunction in cardiovascular diseases: The role of oxidant stress. Circ Res. 2000;87: 4Cai H, Li Z, Goette A, Mera F, Honeycutt C, Feterik K, et al. Downregulation of endocardial nitric oxide synthase expression and nitric oxide production in atrial fibrillation: Potential mechanisms for atrial thrombosis and stroke. Circulation. 2002;106:
, and diabetes likely account in large part for the hypercoagulable state associated with AF.1 However, the observation that markers of coagulation activity increase when the duration of AF is >12 hours suggests that AF per se may contribute to enhancement of coagulation.2. The role of cardiovascular risk factors in decreased NO bioavailability in the coronary vascular endothelium is well established.3 Thus, it is reasonable to speculate that they may also contribute to the downregulation of endocardial NOS.4 However, mechanical factors secondary to disorganized atrial contraction may also play a role.4 Decreased NO bioavailability, in turn, leads to an environment conducive to platelet adhesion to the endocardium and an altered fibrinolytic balance (increased PAI-1). Since activation of the coagulation system with subsequent thrombin formation is the primary pathogenic mechanism, the result is a fibrin-rich clot. 1Feng D, D Agostino RB, Silbershatz H, Lipinska I, Massaro J, Levy D, et al. Hemostatic state and atrial fibrillation (the Framingham Offspring Study). Am J Cardiol. 2001;87: Sohara H, Amitani S, Kurose M, Miyahara K. Atrial fibrillation activates platelets and coagulation in a time-dependent manner: a study in patients with paroxysmal atrial fibrillation. J Am Coll Cardiol. 1997;29: Cai H, Harrison DG. Endothelial dysfunction in cardiovascular diseases: The role of oxidant stress. Circ Res. 2000;87: Cai H, Li Z, Goette A, Mera F, Honeycutt C, Feterik K, et al. Downregulation of endocardial nitric oxide synthase expression and nitric oxide production in atrial fibrillation: Potential mechanisms for atrial thrombosis and stroke. Circulation. 2002;106:")
85
Effect of anticoagulation intensity on post-stroke survival in patients with AF
Content Points: Hylek et al retrospectively studied the frequency and severity of incident ischemic strokes in a cohort of 13,559 patients with AF.1 As shown, the 30-day survival among patients who were not taking warfarin or aspirin when they had an ischemic stroke was significantly worse compared with patients who were on antithrombotic medication (aspirin or warfarin). Survival among patients who were taking warfarin and who had an INR <2.0 was also significantly worse as compared with warfarin patients who had an INR >2.0. Survival among patients who were taking aspirin was comparable to survival among patients who were taking warfarin and who had an INR <2.0. The investigators concluded that INR >2.0 markedly reduces the severity of stroke. 1Hylek EM, Go AS, Chang Y, Jensvold NG, Henault LE, Selby JV, Singer DE. Effect of intensity of oral anticoagulation on stroke severity and mortality in atrial fibrillation. N Engl J Med. 2003;349:
. Survival among patients who were taking warfarin and who had an INR <2.0 was also significantly worse as compared with warfarin patients who had an INR >2.0. Survival among patients who were taking aspirin was comparable to survival among patients who were taking warfarin and who had an INR <2.0. The investigators concluded that INR >2.0 markedly reduces the severity of stroke. 1Hylek EM, Go AS, Chang Y, Jensvold NG, Henault LE, Selby JV, Singer DE. Effect of intensity of oral anticoagulation on stroke severity and mortality in atrial fibrillation. N Engl J Med. 2003;349:")
86
AFFIRM: Effect of anticoagulation intensity on stroke risk
Content Points: The Atrial Fibrillation Follow-up Investigation of Rhythm Management (AFFIRM) results support the critical importance of maintaining a therapeutic anticoagulation level.1 AFFIRM included 4060 patients with recurrent AF that (in the clinical judgment of the investigators) was likely to cause illness or death and warranted long-term treatment. Study subjects were randomized to one of the two treatment strategies and were followed for a mean of 3.5 years with a maximum of 6 years. - In the rhythm control group, continuous anticoagulation was encouraged, but could be stopped if sinus rhythm had been maintained for at least 4 weeks. - In the rate control group, continuous anticoagulation was mandated by the study protocol. Rate control group: As shown, of 77 ischemic strokes, 52 (69%) occurred in patients who had discontinued warfarin or were taking warfarin but had an INR <2.0. Rhythm control group: Of 80 ischemic strokes, 61 (79%) occurred in patients who had discontinued warfarin or were taking warfarin but had an INR <2.0. 1The Atrial Fibrillation Follow-up Investigation of Rhythm Management (AFFIRM) Investigators. A comparison of rate control and rhythm control in patients with atrial fibrillation. N Engl J Med. 2002;347:
 results support the critical importance of maintaining a therapeutic anticoagulation level.1. AFFIRM included 4060 patients with recurrent AF that (in the clinical judgment of the investigators) was likely to cause illness or death and warranted long-term treatment. Study subjects were randomized to one of the two treatment strategies and were followed for a mean of 3.5 years with a maximum of 6 years. - In the rhythm control group, continuous anticoagulation was encouraged, but could be stopped if sinus rhythm had been maintained for at least 4 weeks. - In the rate control group, continuous anticoagulation was mandated by the study protocol. Rate control group: As shown, of 77 ischemic strokes, 52 (69%) occurred in patients who had discontinued warfarin or were taking warfarin but had an INR <2.0. Rhythm control group: Of 80 ischemic strokes, 61 (79%) occurred in patients who had discontinued warfarin or were taking warfarin but had an INR <2.0. 1The Atrial Fibrillation Follow-up Investigation of Rhythm Management (AFFIRM) Investigators. A comparison of rate control and rhythm control in patients with atrial fibrillation. N Engl J Med. 2002;347:")
87
Kardiologia geriatryczna
Nadciśnienie tętnicze Choroba niedokrwienna serca Niewydolność serca Wady serca Migotanie przedsionków

88
Średnie przeżycie w zależności od wyjściowego profilu ryzyka
Prewencja chorób układu krążenia w wieku średnim – zdrowsza starość Arch Intern Med. 2003;163:

Podobne prezentacje