Pobierz prezentację
Pobieranie prezentacji. Proszę czekać

1
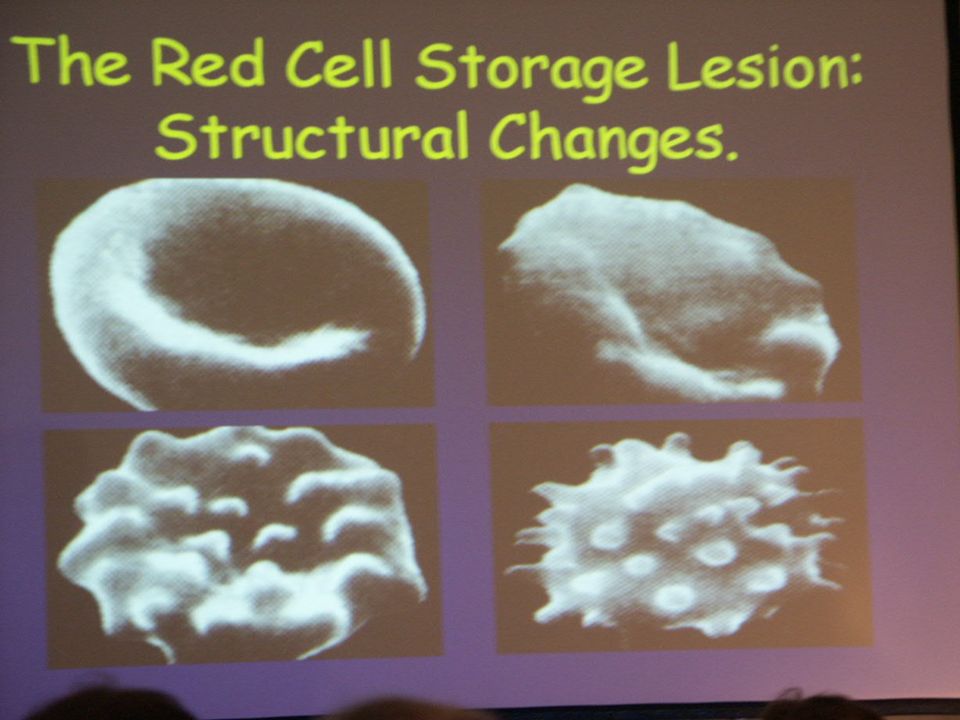
Blood and blood products Indications for transfusion
Janusz Andres

2
What is inside the package?
Whole blood: polivinylochloride bag with antykoagulants and conservants (100 ml in 450 ml) Adenine (50-ties) Today: citric-phosphorate-dextrose
 Adenine (50-ties) Today: citric-phosphorate-dextrose.")
3
Whole blood Additional volume: 1.4-2.5 ml/10 ml blood
Acids (from 3 do 8 g/l) and glucose (ok. 45 g per 100 ml) Besides anticoagulants there are some adjuvants: , phosphate, adenin, guanosin, glukose, mannitol
 and glucose (ok. 45 g per 100 ml) Besides anticoagulants there are some adjuvants: , phosphate, adenin, guanosin, glukose, mannitol.")
4
Whole blood Changes in blood during storing (40C): Na-K pump, K+ may reach 40 mEq/L lub 80 mEq/L after 3-4 weeks of storing (after 42 days 100 mEq/L), pH and ATP/ADP decreases, xantine and hipoxantine increases (reperfusion injury), adeniny – metabolism, citrate - hipotensja
: Na-K pump, K+ may reach 40 mEq/L lub 80 mEq/L after 3-4 weeks of storing (after 42 days 100 mEq/L), pH and ATP/ADP decreases, xantine and hipoxantine increases (reperfusion injury), adeniny – metabolism, citrate - hipotensja.")
5
Whole Blood Leukocytes even after antyleukocytes filters. Leukocytes are alive and induce immunosupression (recipient DNA seen even after year), old blood – increases of: Il6, Il8, TNF alpha (in 28 day level may increase 50 times), bradykinin, C3a, C5a, serotonin
, old blood – increases of: Il6, Il8, TNF alpha (in 28 day level may increase 50 times), bradykinin, C3a, C5a, serotonin.")
6
Whole Blood 70% erythrocytes must be alive (FDA) after 42 days, but after h formation of eichinocytes i and shistocytes (after 30 days 80%) – „reanimated” 24 h after administration Microagregates (from 30 RBC) may induce flow disturbances Decrease in 2,3DPG needs 24 h for Hb to be normal in oxygen delivery
 after 42 days, but after h formation of eichinocytes i and shistocytes (after 30 days 80%) – „reanimated 24 h after administration. Microagregates (from 30 RBC) may induce flow disturbances. Decrease in 2,3DPG needs 24 h for Hb to be normal in oxygen delivery.")
8
Risk factors in 90-ties Infections Viral Frequency/unit death/milion
Hepatitis A 1 / Hepatitis B 1 / – 1/ ,14 Hepatitis C 1 / 30 – 1 / <0.5 HIV 1 / – 1/ <0,5 Parvovirus B19 1/

9
Current frequency of risk
HIV - 1: HBV – 1: HCV – 1 : Bakterie – 1 : vCJD – published

10
Risk factors Immunological complications cardiac- and thoracic surgery
Linear increase in infection rate in gastrointestinal, cardiac- and thoracic surgery Increase lenght of stay in ICU Cost increase Cancer disease

11
Risk factors Immunological complications
Hemolytic reactions 1 / Delayed hemolytic reaction 1 / 1 000 TRALI ? Transfusion-related acute lung injury

12
Transfusion-related acute lung injury
T R A L I Transfusion-related acute lung injury Signs after 2-4 h Dyspnea Hipotention Increase in temperature Pulmonary oedema 1 / Unit transfused Antyleucocytes antibody Predisposing factors: infections surgery massive transfusions

13
FFP No erythrocytes, no metabolism
1 U FFP (200 ml): 400 mg fibrynogen and 1 UA/ml clothing factors V,VII most unstable Very complicated scanning system for viruses Crioprecypitat: 180 mg fibrynogen (20 ml), factor VIII U
: 400 mg fibrynogen and 1 UA/ml clothing factors. V,VII most unstable. Very complicated scanning system for viruses. Crioprecypitat: 180 mg fibrynogen (20 ml), factor VIII U.")
14
Indications for FFP transfusion
Massive blood transfusion > 1 blood volume or > 10 U./24 godz. + hemorrage + increase in PT, INR or aPTT DIC active hemorrage + PT, INR lub aPTT

15
FFP transfusions (2) Vit. K deficiency Anticoagulant therapy
Liver injury + PT, INR, aPTT > 1,5x Serious bleeding Surgery Invasive diagnostic procedures

16
Contraindication for FFP transfusions
Volume replacement Hypoalbuminemia and/or nutrition problem Hypogammaglobulinemia Hemofilia and/or von Willebrandta Syndrome Genetic disorders (clothing factor deficiency)
")
17
Platelets 1 U consists with 5.5 x 1010 platelets w 50 ml of plasma (1 U „aphoresis” 30 x 1010) Storage in 22oC 5 days (in 4 0C plts dying) Only 40-60% platelets are active (no nucleus, apoptosis) Interactions with leukocytes and cytokines (stroke)
 Interactions with leukocytes and cytokines (stroke)")
18
Indications for platelets infusion
< x 10 9/L with active bleeding and/or risk of bleeding < 10 x 10 9/L always Expected effect: 5 x 10 9/L increase for 1 Unit transfused. HIT

19
Posttransfusion reactions
Shock and hemolysis Delayed hemolysis Fever Allergy Volume overload Pulmonary oedema Sepsis Thrombocytopenia „Graft versus host reaction”

20
There is a risk asssocieted with blood and blood products transfusion
Conclusion 1 There is a risk asssocieted with blood and blood products transfusion

21
When we have to transfuse?
Hemodynamic instability Lost of blood Hemoglobin level

22
Clinical scenario TRANSFUSION: what? Hypovolemia Injury (bleeding?)
Diagnosis of bleeding Tachycardia Low blood pressure Bad peripheral perfusion Low diuresis TRANSFUSION: what? Hypovolemia Stress reaction – catecholamin overshoot Oxygen transport disturbances

23
Compensations mechanisms in DO2 in anaemia
Blood viscosity * SVR * venous return CO (up to Ht 30% no additional work for the heart) * tachycardia * contactility tissue O2 extraction * right shift of the Hb oxygenation curve * level of 2,3-diphosphogliceride in erythrocytes
 * tachycardia. * contactility. tissue O2 extraction. * right shift of the Hb oxygenation curve. * level of 2,3-diphosphogliceride in. erythrocytes.")
24
Goal Directed Therapy Rivers 2001
ScvO2 > 70% increses survival in sepsis Do we have GDT in blood transfusion? What kind of goals? ScvO2, lactate, DO2?

25
Physiology and pathology
DO2 = CI x Hb x Sa02 x 13.9 (ml/min/m2) Norma = 3 x 12 x x 13.9 = 500 Anemia = 6x 6 x x 13.9 = 500 Hipoksemia= 6 x 12 x 0.48 x 13.6 = 500 Low output syndrome = 1.5 x 12 x 0.96 x 13.6 = 250
 Norma = 3 x 12 x 0.96 x 13.9 = 500. Anemia = 6x 6 x 0.96 x 13.9 = 500. Hipoksemia= 6 x 12 x 0.48 x 13.6 = 500. Low output syndrome = 1.5 x 12 x 0.96 x 13.6 = 250.")
26
Oxygenation/Saturation
exercise CO SvcO2=SaO2 – (VO2/CI x Hb x 13.9) hipoxaemia anaemia
 hipoxaemia anaemia.")
27
Physiology and pathology
V02=CI x Hg x (Sa02 – Sv02) x 13.9 norma=3 x 12 x ( ) x 13.9=125 anemia=4.5x 6 x ( ) x 13.9=125 hipoksemia=6x 12 x ( )x13.9=125 low output=1.5x 12 x ( )x13.9=125 exercises=4.5x12x ( )x13.9=250
 x norma=3 x 12 x ( ) x 13.9=125. anemia=4.5x 6 x ( ) x 13.9=125. hipoksemia=6x 12 x ( )x13.9=125. low output=1.5x 12 x ( )x13.9=125. exercises=4.5x12x ( )x13.9=250.")
28
Do we need blood for critical care pts
Do we need blood for critical care pts? Napolitano LM, Crit Care M, 2004 Are there signs of oxygenation improvement? Do transfusions really decrease mortality? What about the age of blood? When transfusions cause increase in mortality?

29
Conclusion 2 The clinical scenario and individual patient conditions are decision making factors not the Hb level

30
Viele MK, Weiskopf RB., Transfusion 1994;43:396-401.
54 publications, 134 patients Hb 5 – 8 g% no mortality due to anaemia Hb < 5 g% - mortality rate 37%

31
Hebert PC. et al., JAMA 1999; 340: Group I - transfusion restriction (n=418) Hb g% mortality: 77 pts (18%) Grupa II – liberal strategy (n=420) Hb 10 – 12 g% mortality: 101 pts (24%) APACHE II < 20 p. and pts < 55 years old – mortality decreases about 50% in gr.I
 Hb 10 – 12 g% mortality: 101 pts (24%) APACHE II < 20 p. and pts < 55 years old – mortality decreases about 50% in gr.I.")
32
Criteria TRICC (Canada) Hebert P.C. et. al. TATM 2002,2,15
Hb 8.5 g/l versus 10.5 g/l in two groups Cardiac diseases (278 pts) and artificial ventilation (714 pts) Eccept pts with MI and unstable CAD transfusion trigger Hb 7 g% is save in both groups
 and artificial ventilation (714 pts) Eccept pts with MI and unstable CAD transfusion trigger Hb 7 g% is save in both groups.")
33
Increase risk of hypoxaemia
Age (> 65 lat) Cardiovascular and pulmonary diseases Cerebrovascular diseases
 Cardiovascular and pulmonary diseases. Cerebrovascular diseases.")
34
Pts > 65 year with MI treated nonivasively
Wu W.C. et al.NEJM 2001,345, pts: Low Ht at admission– increase mortality Ht 30-33% + transfusion = better outcome Ht > 36% +transfusion = higher mortality rate

35
Rao JAMA 2004, 1555-1562 PTS with MI and acute coronary syndrome
Blood transfusion in pts with Ht > 33% increases mortality The best results of transfusion in pts with Hg 8 – 9 g%

36
ICU pts blood transfusion indications: Marcucci C. 2005 Yearbook of IC
1. Except 2,3,4: Hg 6g%, PvO2<32mmHg, Ex02>50% 2. Pts > 80 age: Hg 7g% 3. CAD: Hg 8g% 4. CNS, fever: Hg 7g%

37
ASA Guidelines Rare indications with Hb > 10 g% and almost always with Hb < 6 g% Hb g% decision make upon: Risk of inadequate oxygenation Rate of bleeding Cardiopulmonary status of the patient Oxygen consumption/ requirements

38
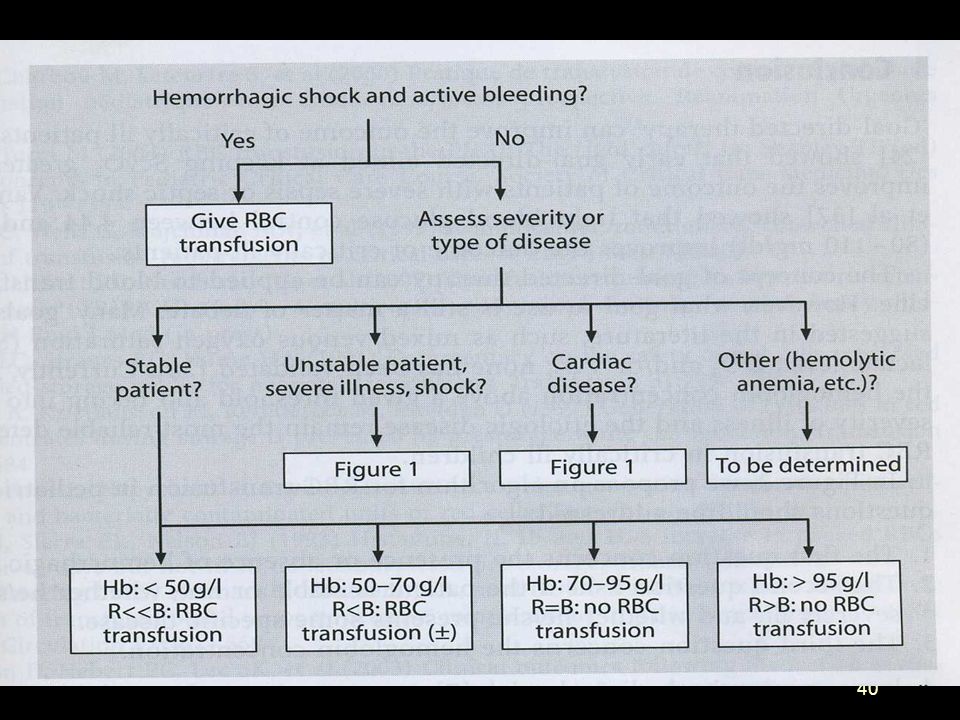
When? Hb < 6 g% yes Hb > 10 g% no Hb 6 – 10 g% ?

39
Patients with advanced age
Conclusion 3 Patients with advanced age and cardio-pulmonary deseases, fever, unstable or critical state require individual assesments indications for blood transfusions

42
Thanks for your attention

44
Wniosek końcowy (Hebert 2005)
Przetaczamy krew od poziomu Hg 7g% (70 g/L) Pacjenci w stanach krytycznych powinni mieć poziom Hg 7 – 9 g% ( g/L)
 Pacjenci w stanach krytycznych powinni mieć poziom Hg 7 – 9 g% ( g/L)")
45
Jak leczyć ostrą utratę krwi w kardiochirurgii?
„Protamine” „Prolene” „Platelets” „Plasma” rFVIIa (NovoSeven) „Prayer”
 „Prayer")
46
Fakty fizjologiczne Anemia: wpływa na krzywą dysocjacji, wzrost CO, SV, HR, wzrost aktywności układu współczulnego, obniżenie oporów obwodowych, redystrybucja przepływu, wzrost przepływu mózgowego i wieńcowego, obniżenie kurczliwości m. sercowego u chorego z chorobą wieńcową

47
Farmakologiczne metody
Aprotynina (Trascolan) Kwas epsilon-aminokapronowy Kwas tranexamowy Operacje serca, wątroby, ortopedyczne,
 Kwas epsilon-aminokapronowy. Kwas tranexamowy. Operacje serca, wątroby, ortopedyczne,")
49
Hebert PC NEJM 1999, 340,409-417 Opcja restrykcyjna ?
Cel: Poziom hemoglobiny 7-9 g/dl (8,5+-0,7) Przetoczono 2,6 (+-4) j kkcz Uniknięto transfuzji u 33 % chorych Opcja liberalna ? Cel: Poziom hemoglobiny g/dl (11,2+-0,7) Przetoczono 5,6 (+-5,3) j kkcz Nie uniknięto transfuzji 900 chorych
 Przetoczono 2,6 (+-4) j kkcz. Uniknięto transfuzji u 33 % chorych. Opcja liberalna Cel: Poziom hemoglobiny g/dl (11,2+-0,7) Przetoczono 5,6 (+-5,3) j kkcz. Nie uniknięto transfuzji. 900 chorych.")
50
Wskaźniki transportu tlenu
PvO2 SvO2 < 55% Paone G. Silverman N.A.; Circulation 1997; 96(suppl 9): II VO2 O2 ER (CaO2 – CvO2)/CaO2 > 50% stęż. mleczanów
: II VO2. O2 ER (CaO2 – CvO2)/CaO2. > 50% stęż. mleczanów.")
51
Optymalizacja wolemii
Normowolemia Normotermia Prawidłowe krzepnięcie Krystaloidy „sprzyjają” krzepnięciu Preparaty oparte na żelatynie mniej upośledzają krzepnięcie niż koloidy skrobiowe

52
Postępowanie śródoperacyjne w ostrym krwotoku
Brak wskazań do uzyskania poziomu wyjściowego Hb Utrzymywać normowolemię i normotermię (hipotermia upośledza funkcję płytek, nasila krwawienie i częstość infekcji po operacjach brzusznych) Stosować mieszaninę hiperoksyczną Optymalizować terapię płynową (krystaloidy przyśpieszają krzepnięcie)
 Stosować mieszaninę hiperoksyczną. Optymalizować terapię płynową (krystaloidy przyśpieszają krzepnięcie)")
53
Skurczowe - - obniżone b.niskie
I II III IV Utrata krwi(ml) Procent < >40 Objętość >2000 Ciśnienie Skurczowe obniżone b.niskie Rozkurczowe zwiększone obniżone b niskie Tętno >120 Powrót normalny wolny >2s wolny >2s brak Włośniczkowy Oddech normaln normalny >20/min >20/min Diureza(ml/h) > 30 ml Stan mentalny przytomny niedotleniony niedotleniony nieprzytomny pobudzony podsypiający
 Procent < >40. Objętość >2000. Ciśnienie. Skurczowe - - obniżone b.niskie. Rozkurczowe - zwiększone obniżone b niskie. Tętno >120. Powrót normalny wolny >2s wolny >2s brak. Włośniczkowy. Oddech normaln normalny >20/min >20/min. Diureza(ml/h) > 30 ml Stan mentalny przytomny niedotleniony niedotleniony nieprzytomny. pobudzony podsypiający.")
54
hemodilucja normowolemiczna do Hb 5g% (po 2 i 4 h)
Badania wpływu anemii na ochotnikach Weiskopf RB i wsp. JAMA 1998; 279: Przytomni, zdrowi pacjenci przed zabiegiem chirurgicznym (n=11) + zdrowi ochotnicy (n=21) hemodilucja normowolemiczna do Hb 5g% (po 2 i 4 h) nie stwierdzono cech niedotlenienia tkankowego (cewnik SG, Holter, poziom mleczanów)
 + zdrowi ochotnicy (n=21) hemodilucja normowolemiczna do Hb 5g% (po 2 i 4 h) nie stwierdzono cech niedotlenienia tkankowego (cewnik SG, Holter, poziom mleczanów)")
55
„Będziesz potępiony jeżeli to zrobisz, będziesz potępiony jeżeli tego nie zrobisz” CCM 2005 Spiess
Habib i wsp. CCM 2005: zarówno anemia (poniżej 8 g%), jak i wczesne (w czasie CPB) przetoczenia krwi powodują wzrost powikłań: niewydolności nerek , pobytu w szpitalu i śmiertelności
, jak i wczesne (w czasie CPB) przetoczenia krwi powodują wzrost powikłań: niewydolności nerek , pobytu w szpitalu i śmiertelności.")
56
Predonacja: koszty, szkolenie personelu, duże marnotrastwo
Okołooperacyjne odzyskiwanie, zmniejszanie strat i ochrona WŁASNEJ KRWI Predonacja: koszty, szkolenie personelu, duże marnotrastwo Hemodilucja normowolemiczna: obciążenie płynami, rozcieńczenie czynników krzepnięcia, „logistyka” Reinfuzja krwi wynaczynionej: koszty, zakażenia, sprzęt

57
Świadkowie Jehowy 1872, USA ok. 6 mln wyznawców w 230 krajach, 8 mln sympatyków 1945 stanowisko co do niektórych zabiegów i procedur medycznych Chory nieprzytomny Dziecko (poniżej 16 roku życia) Osoba w wieku lat
 Osoba w wieku lat.")
58
Świadkowie Jehowy Służba Informacji o Szpitalach w Polsce
Towarzystwo Strażnica ul Warszawska 14 Nadarzyn tel.: Fax:

59
Erytropoetyna w OIT 1988 Niedokrwistość u chorych w OIT spowodowana niedoborem EPO Corvin HL et al. CCM 1999, 27, , podawanie EPO (rHuEPO) 300 IU/kg istotnie zmniejsza przetoczenia Koszty terapii mogą być porównywalne z krwią (400 USD w USA)
 300 IU/kg istotnie zmniejsza przetoczenia. Koszty terapii mogą być porównywalne z krwią (400 USD w USA)")
60
Cena krwi Od stycznia 1999 roku odpłatność za krew
Koszty RCKiK/ilość jednostek dostarczana= cena W Polsce pobiera się ok jednostek krwi rocznie Opłata wynosi 140 mln złotych (srednio 178 zł za jednostkę (różnice o 100%) Koszty hemodylucji i predonacji powinny być mniejsze Cena cell savera zwraca się po częstym używaniu (400 razy w ciągu roku)
 Koszty hemodylucji i predonacji powinny być mniejsze. Cena cell savera zwraca się po częstym używaniu (400 razy w ciągu roku)")
61
Wniosek Pomimo upływu 104 od poczatków transfuzjologii nie znamy odpowiedzi na dwa zasadnicze pytania: 1. Czy przetoczenie krwi dostarcza tlenu? 2. Czy przetoczenie krwi wpływa na wyniki leczenia?

62
„Będziesz potępiony jeżeli to zrobisz, i będziesz potępiony jeżeli tego nie zrobisz”

Podobne prezentacje












 Warsaw University of Life.>")







