Pobierz prezentację
1
GENETYKA W ONKOLOGII – ASPEKTY MEDYCZNE I EKONOMICZNE J. Lubiński INTERNATIONAL HEREDITARY CANCER CENTER POMERANIAN MEDICAL UNIVERSITY READGENE SA Warszawa 25.10.2011 r.

2
If we want to solve problem / be successful we need to: a) work hard and wise b) be lucky If we want to solve problem / be successful we need to: a) work hard and wise b) be lucky
 work hard and wise b) be lucky If we want to solve problem / be successful we need to: a) work hard and wise b) be lucky")
3
~38 mln country with high level of genetic homogeneity Luck!!! Poland

5
Górski B. et al. AJHG, June 2000

6
POLISH FAMILIES WITH STRONG AGGREGATION OF BREAST/OVARIAN CANCERS (n=200) BRCA 1 ~65% BRCA2~4% BRCA 1 ~65% BRCA2~4% Górski B. et al. Int. J. Can, 2004

7
POLISH PANEL OF BRCA1 MUTATIONS 5382 ins C C 61 G 4153 del A 5382 ins C C 61 G 4153 del A 90% of mutations Górski B. et al. Int. J. Can, 2004

8
BRCA1 FOUNDER MUTATIONS IN POLAND GÓRSKI B. ET AL. - PATENT NO P335917 - MULTIPLEX PCR - 50€

9
A. BRCA1 PROPHYLACTICS RISK BR OV RISK BR OV Oral contraceptives 30yrs 0.5 Breast feeding > 1 yrs 0.5 Later menarche per yr 0.9 Tubal ligation 0.5 Adnexectomy 0.2 0.05 Tamoxifen 0.5 Adnexectomy + tamoxifen 0.15 Mastectomy 0.01 RISK BR OV RISK BR OV Oral contraceptives 30yrs 0.5 Breast feeding > 1 yrs 0.5 Later menarche per yr 0.9 Tubal ligation 0.5 Adnexectomy 0.2 0.05 Tamoxifen 0.5 Adnexectomy + tamoxifen 0.15 Mastectomy 0.01

10
DETECTION OF EARLY BREAST CANCERS IN BRCA1 MUTATION CARRIERS USGMAMMOGR.MRI ~20%~20%~90% USGMAMMOGR.MRI ~20%~20%~90% Narod S. et al. 2003 Scientific background

11
Prophylactic adnexectomy Tamoxifen Chemotherapy Prophylactic adnexectomy Tamoxifen Chemotherapy DIFFERENCES IN TREATMENT OF BRCA1 BREAST CANCERS

12
MSH2 / MLH1 tests In families matching the following criteria: CRC + CRC END SB UR. TR. ≥1 of cancers DGN < 50 yrs In families matching the following criteria: CRC + CRC END SB UR. TR. ≥1 of cancers DGN < 50 yrs

13
FEATURES MODIFYING RISK OF COLORECTAL CANCER IN CARRIERS OF MSH2/MLH1 MUTATION BEGININGEVERY BEGININGEVERY COLOSCOPY WITH POLYPECTOMY 25 YRS 2 YRS INTRAVAGINAL USG 35 YRS 1 YRS RISK FROM 80% TO 30% DETECTION OF EARLY CANCERS BEGININGEVERY BEGININGEVERY COLOSCOPY WITH POLYPECTOMY 25 YRS 2 YRS INTRAVAGINAL USG 35 YRS 1 YRS RISK FROM 80% TO 30% DETECTION OF EARLY CANCERS

14
POPULATION SCREENINGS IN POLAND 4% (~200) of BRCA1 carriers among 5000 relatives of women with breast cancer dgn < 50 yrs or ovarian cancer dgn at any age Thanks to geneticists - oncologists from 20 Polish centers! 4% (~200) of BRCA1 carriers among 5000 relatives of women with breast cancer dgn < 50 yrs or ovarian cancer dgn at any age Thanks to geneticists - oncologists from 20 Polish centers!
 of BRCA1 carriers among 5000 relatives of women with breast cancer dgn < 50 yrs or ovarian cancer dgn at any age Thanks to geneticists - oncologists from 20 Polish centers!.")
15
WEST-POMERANIA REGION JANUARY 2001 – MAY 2002 1,258 mln questionaires out of 1,45 mln of inhabitants the first worldwide large screening for hereditary cancers 1,258 mln questionaires out of 1,45 mln of inhabitants the first worldwide large screening for hereditary cancers POPULATION SCREENINGS IN POLAND

16
BRCA 1 MUTATION DETECTION COST750 € SURVEILLANCE COST1650 € (USG, MAMMOGRAPHY, FNAB, ADNEXECTOMY, TAMOXIFEN) RISK REDUCTION BREAST60% 10% (WITHOUT PROPHYLACTIC MASTECTOMY) OVARY40% 5% MUTATION DETECTION COST750 € SURVEILLANCE COST1650 € (USG, MAMMOGRAPHY, FNAB, ADNEXECTOMY, TAMOXIFEN) RISK REDUCTION BREAST60% 10% (WITHOUT PROPHYLACTIC MASTECTOMY) OVARY40% 5% POPULATION SCREENINGS IN POLAND
 RISK REDUCTION BREAST60% 10% (WITHOUT PROPHYLACTIC MASTECTOMY) OVARY40% 5% MUTATION DETECTION COST750 € SURVEILLANCE COST1650 € (USG, MAMMOGRAPHY, FNAB, ADNEXECTOMY, TAMOXIFEN) RISK REDUCTION BREAST60% 10% (WITHOUT PROPHYLACTIC MASTECTOMY) OVARY40% 5% POPULATION SCREENINGS IN POLAND")
17
2000-2003 BRCA1 mutation carriers with breast/ovarian cancers N=50 Treatment costs~5 500 € Social security costs~8 800 € GP per capita lost~50 000 € ~64 300 € ~64 300 € Average annual cost~16 000 € Treatment costs~5 500 € Social security costs~8 800 € GP per capita lost~50 000 € ~64 300 € ~64 300 € Average annual cost~16 000 € Marska N, US 2004 COMPELLING ECONOMICS OF PREVENTION

18
Family history DNA tests BRCA1 BRCA1 BRCA2 BRCA2 CHEK2 – homozygotes – htr + FH – BRCA2 (5972 C/T) CHEK2 – homozygotes – htr + FH – BRCA2 (5972 C/T) ATM ATM Family history DNA tests BRCA1 BRCA1 BRCA2 BRCA2 CHEK2 – homozygotes – htr + FH – BRCA2 (5972 C/T) CHEK2 – homozygotes – htr + FH – BRCA2 (5972 C/T) ATM ATM High penetrance/risk – breast ca
 CHEK2 – homozygotes – htr + FH – BRCA2 (5972 C/T) ATM ATM Family history DNA tests BRCA1 BRCA1 BRCA2 BRCA2 CHEK2 – homozygotes – htr + FH – BRCA2 (5972 C/T) CHEK2 – homozygotes – htr + FH – BRCA2 (5972 C/T) ATM ATM High penetrance/risk – breast ca")
20
NATIONAL PROGRAMME URGENTLY NEEDED!!!

21
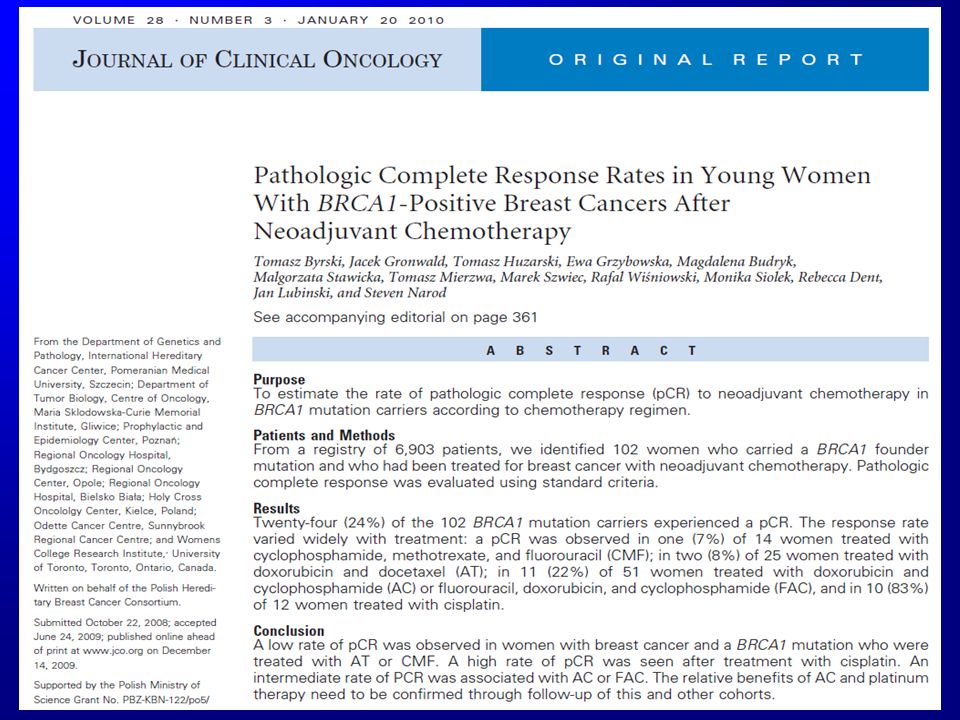
2.Complete remission of BRCA1 – dependant breast cancers using Cis-platinum Milestone discoveries International Hereditary Cancer Center 2008/9

22
44 patients 15 (+) – 10/15 pCR – 67% 29 (−) – 24/29 pCR – 83% 44 patients 15 (+) – 10/15 pCR – 67% 29 (−) – 24/29 pCR – 83% BRCA1-dependendnt breast cancer Preoperative treatment
 – 10/15 pCR – 67% 29 (−) – 24/29 pCR – 83% 44 patients 15 (+) – 10/15 pCR – 67% 29 (−) – 24/29 pCR – 83% BRCA1-dependendnt breast cancer Preoperative treatment")
23
Retrospective analysis neoadjuvant treatment of 141 consecutive BRCA1 mutation carriers with diagnosis of breast cancer < 51 yrs (n=7000) Retrospective analysis neoadjuvant treatment of 141 consecutive BRCA1 mutation carriers with diagnosis of breast cancer < 51 yrs (n=7000)
 Retrospective analysis neoadjuvant treatment of 141 consecutive BRCA1 mutation carriers with diagnosis of breast cancer < 51 yrs (n=7000)")
25
Neo-adjuvant treatment of breast cancer – complete pathologic remission > 95% of five year survival ! Neo-adjuvant treatment of breast cancer – complete pathologic remission > 95% of five year survival ! CHEMOTHERAPYCHEMOTHERAPY

26
METASTATIC STUDY BRCA1 – dependent BC

27
Response to treatment ResponseNumber Evidence of progression Months since initiation of treatment,* mean Number deceased Complete 9629.32 Partial 7427.65 Stable disease 3313.63 Progressive 116.01 From date of first treatment untill July 31, 2011 if alive, or untill date of death, if dead Byrski T et al.

28
CONCLUSIONSCONCLUSIONS 1.Platinum-based chemotherapy is effective in a high proportion of patients with BRCA1-associated breast cancers 2.BRCA1 testing is a critical issue for choice of breast cancer treatment 3.Validating studies needed 1.Platinum-based chemotherapy is effective in a high proportion of patients with BRCA1-associated breast cancers 2.BRCA1 testing is a critical issue for choice of breast cancer treatment 3.Validating studies needed

29
Milestone discoveries Cancer chemoprevention using selenium International Hereditary Cancer Center 2011

30
Stężenia Se w diecie / organizmie? Osobnicze różnice w genotypach? Stężenia Se w diecie / organizmie? Osobnicze różnice w genotypach? Przyczyny dotychczasowych niepowodzeń

31
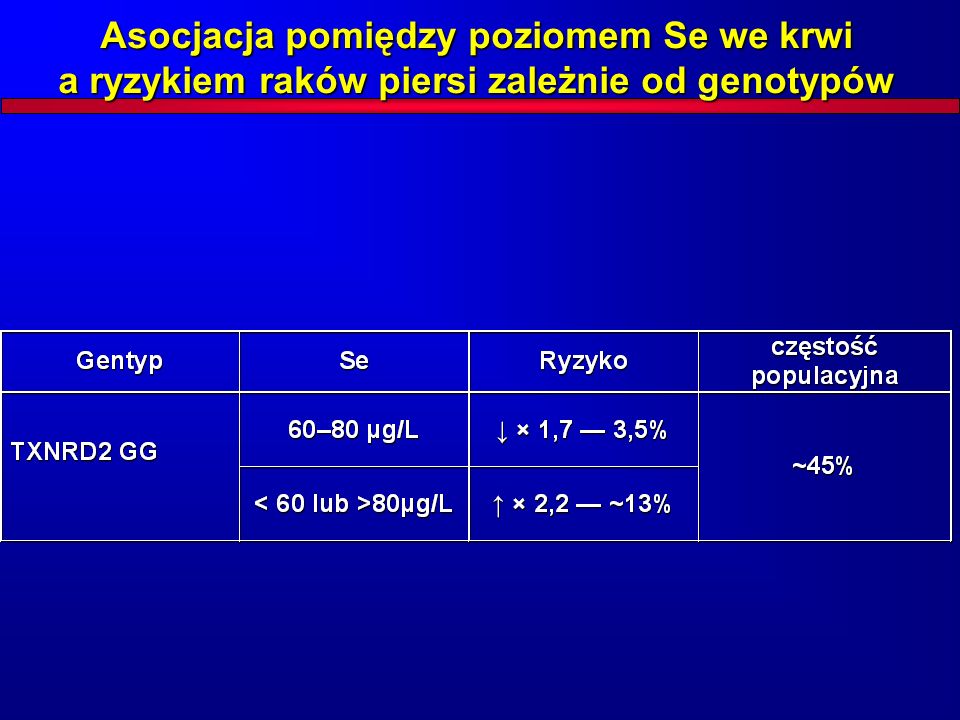
Asocjacja pomiędzy poziomem Se we krwi a ryzykiem raków piersi zależnie od genotypów a) Kolejne raki piersi b) Raki piersi u nosicielek mutacji BRCA1
 Kolejne raki piersi b) Raki piersi u nosicielek mutacji BRCA1")
32
Asocjacja pomiędzy poziomem Se we krwi a ryzykiem raków piersi zależnie od genotypów

34
Asocjacja pomiędzy poziomem Se we krwi a ryzykiem raków płuca i krtani niezależnie od genotypów

35
I vs IV ćwiartka p<0.0001 OR 13.2 CI 4.6-37.6 Se 90-110 μg/l 0/15 !!! p 90-110 μg/l 0/15 !!! p<0.0001 OR 125.8 I vs IV ćwiartka p<0.0001 OR 13.2 CI 4.6-37.6 Se 90-110 μg/l 0/15 !!! p 90-110 μg/l 0/15 !!! p<0.0001 OR 125.8 Rak płuca

36
Ryzyko raka płuca a stężenie selenu we krwi 0 1 2 3 4 5 6 020406080100120140160180200 PolskaUSA Ryzyko stężenie Se [μg/l]
![Ryzyko raka płuca a stężenie selenu we krwi PolskaUSA Ryzyko stężenie Se [μg/l]](http://images.slideplayer.pl/35/10507376/slides/slide_36.jpg "Ryzyko raka płuca a stężenie selenu we krwi PolskaUSA Ryzyko stężenie Se [μg/l]")
37
Wniosek – podsumowanie Poziom selenu markerem grup ryzyka raków tytoniozależnych np. kwalifikacja do TK płuc? optymalizacja poziomu selenu – kilkakrotne obniżenie ryzyka raków tytoniozależnych? Poziom selenu markerem grup ryzyka raków tytoniozależnych np. kwalifikacja do TK płuc? optymalizacja poziomu selenu – kilkakrotne obniżenie ryzyka raków tytoniozależnych?

38
Wniosek – podsumowanie Genetyka w onkologii – wielki innowacyjny potencjał do wdrożenia zwłaszcza w POLSCE

39
ECONOMICAL CRISIS APPLIED RESEARCH COMMERCIALISATION – SPIN OFFS READ GENE SA

40
Main task: global leadership in cancer chemoprevention

41
www.hccpjournal.com
42
Welcome for collaboration…