Pobierz prezentację
Pobieranie prezentacji. Proszę czekać

1
Uszkodzenie nerek u chorego na cukrzycę – nowości patogenetyczne Marian Klinger Katedra i Klinika Nefrologii i Medycyny Transplantacyjnej Uniwersytetu Medycznego we Wrocławiu

2
Patogeneza cukrzycowego uszkodzenia nerek hiperglikemia czynniki hemodynamiczne reakcja zapalna zróżnicowane, wielogenowe podłoże

3
Rozwój uszkodzenia nerek w cukrzycy Kimberly Reidy et al., Molecular mechanisms of diabetic kidney disease. J Clin Invest. 2014;124(6):2333–2340
:2333–2340.")
4
Pathogenesis of kidney disease in patients with diabetes. Hemodynamic and metabolic factors, with a central role for chronic hyperglycaemia, have pivotal roles in the pathophysiology of diabetic nephropathy. Muskiet, M. H. A. et al. Nat. Rev. Nephrol. 10, 88–103 (2014);
;.")
5
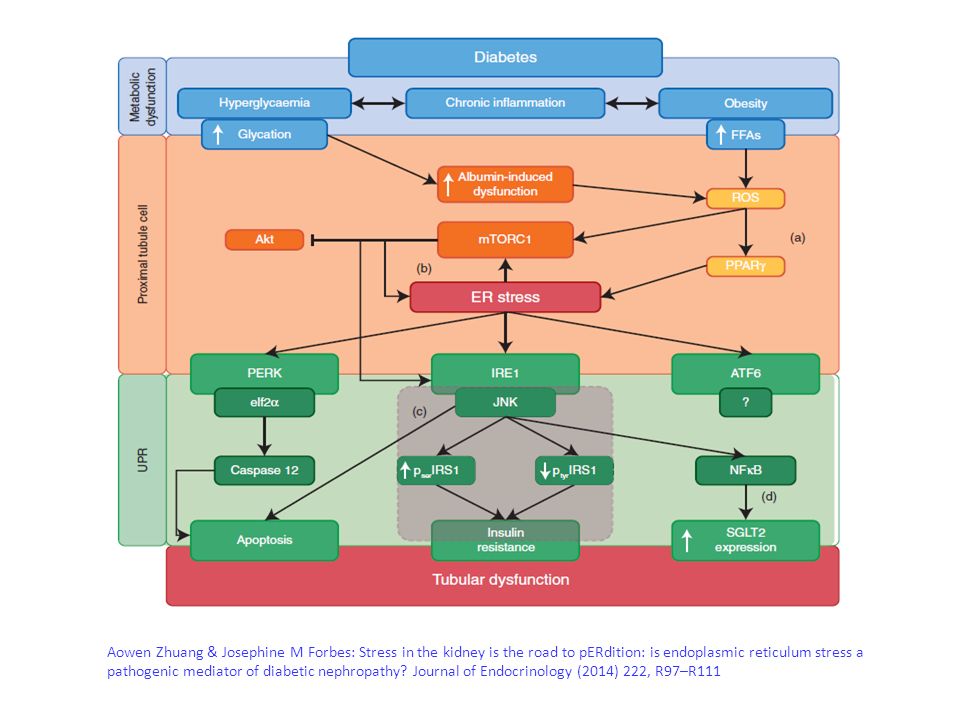
Aowen Zhuang & Josephine M Forbes: Stress in the kidney is the road to pERdition: is endoplasmic reticulum stress a pathogenic mediator of diabetic nephropathy? Journal of Endocrinology (2014) 222, R97–R111
 222, R97–R111.")
7
García-García PM, Getino-Melián MA, Domínguez-Pimentel V,Navarro-González JF. Inflammation in diabetic kidney disease. World J Diabetes 2014; 5(4): 431-443
:")
8
Kimberly Reidy et al. J Clin Invest. 2014; 124(6):2333–2340 Molecular mechanisms of diabetic kidney disease
:2333–2340 Molecular mechanisms of diabetic kidney disease.")
9
[Tang Z.-H., Fang Z. and Zhou L. 2013 Human genetics of diabetic vascular complications. J. Genet. 92, 677–694] Zaburzenia ekspresji genów

10
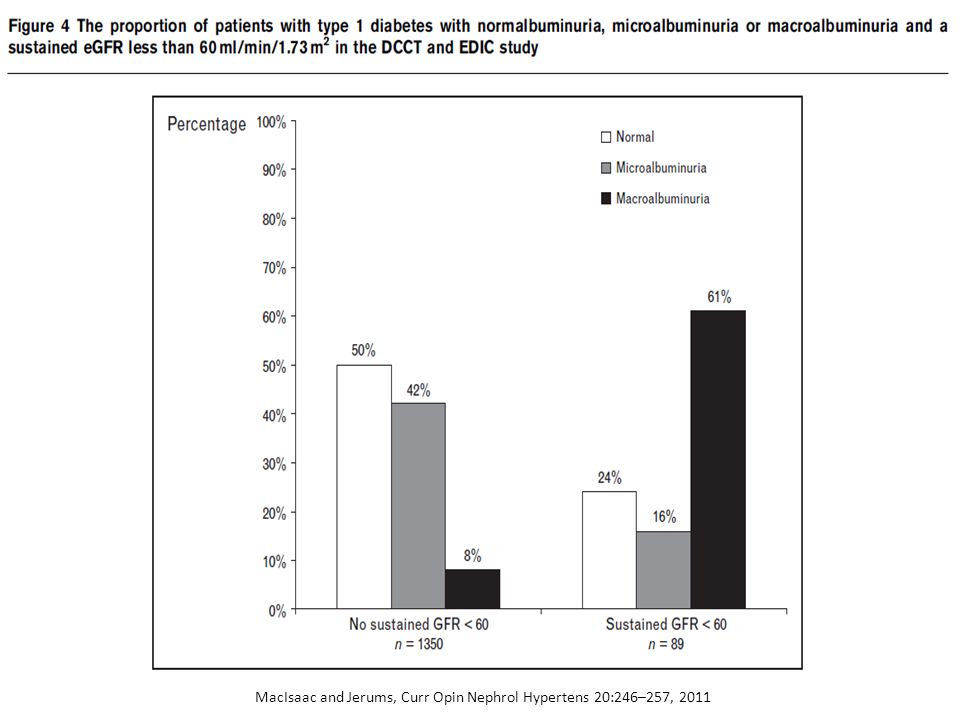
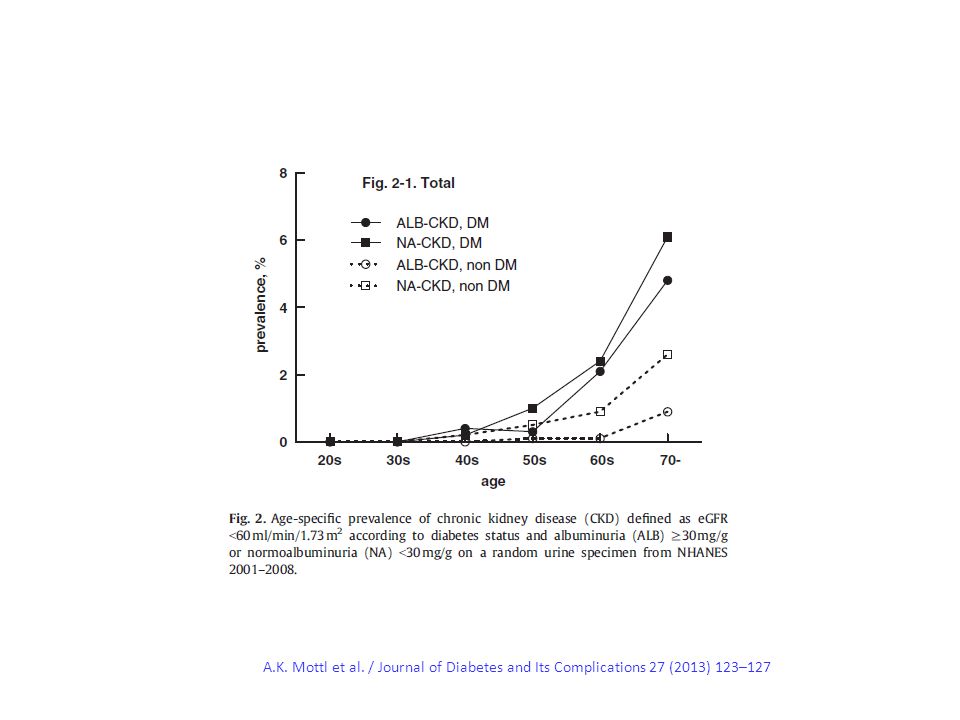
Diabetic kidney disease with and without albuminuria Richard J. Mac Isaac and George Jerums Current Opinion in Nephrology and Hypertension 2011, 20:246– 257 Summary The conventional paradigm of kidney disease in people with diabetes has been challenged. Changes in AER and GFR are being increasingly recognized as complementary rather than obligatory manifestations of diabetic CKD Cukrzycowe uszkodzenie nerek bez białkomoczu; Nie wszystko zależy od podocyta

11
Klasyczny przebieg uszkodzenia nerek w cukrzycy typu 1 MacIsaac and Jerums, Curr Opin Nephrol Hypertens 20:246–257, 2011

12
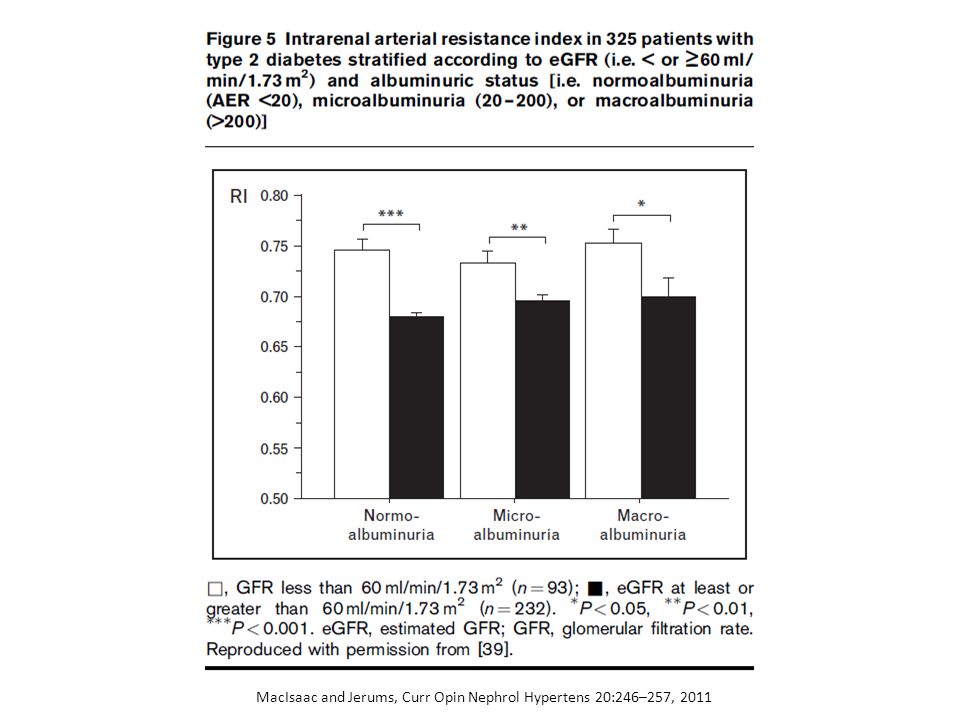
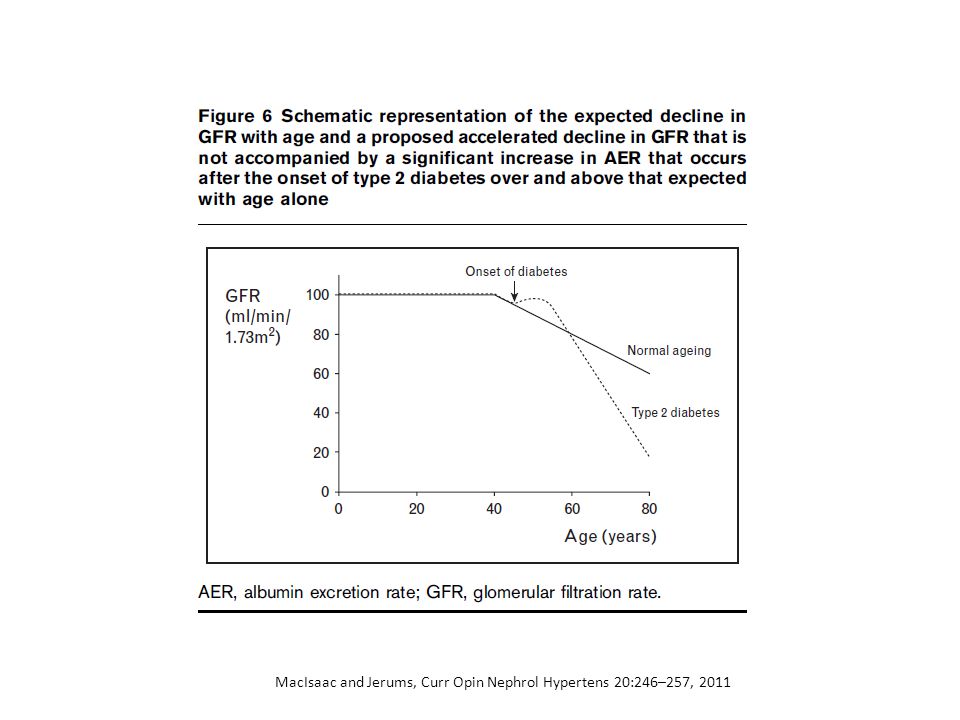
Klasyczny przebieg uszkodzenia nerek w cukrzycy typu 2 MacIsaac and Jerums, Curr Opin Nephrol Hypertens 20:246–257, 2011

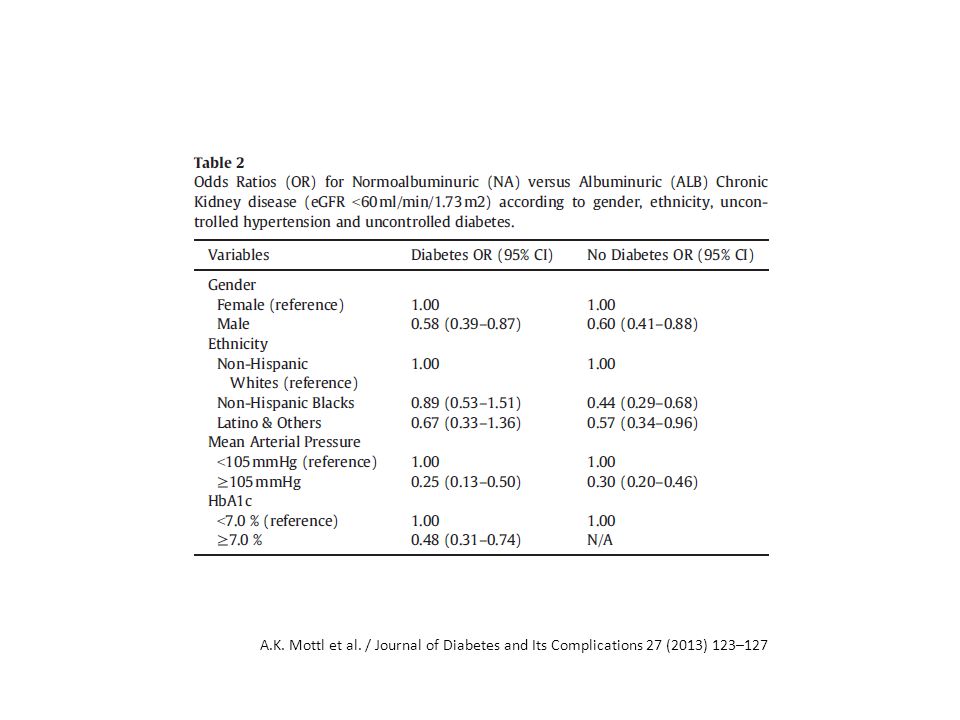
16
A.K. Mottl et al. / Journal of Diabetes and Its Complications 27 (2013) 123–127
 123–127")
19
Odrębności obrazu patofizjologicznego i klinicznego uszkodzenia nerek w cukrzycy typu 1 i 2

20
CKD in the elderly diabetic population may frequently lack proteinuria and therefore be less responsive to RAS blockade. In NHANES III, a third of those surveyed with type 2 diabetes aged 60 to 70 years and with normal urinary albumin excretion nonetheless had a GFR of less than 30 mL/min, and almost half were between 30 and 60 mL/min. Diabetic Kidney Disease in Elderly Individuals Williams, Med Clin N Am 97 (2013) 75–89
 75–89.")
21
Median Glycated Hemoglobin Levels at Each Study Visit The Action to Control Cardiovascular Risk in Diabetes Study Group. N Engl J Med 2008;358:2545-2559

22
10,251 patients (mean age, 62.2 years) The primary outcome was a composite of nonfatal myocardial infarction, nonfatal stroke, or death from cardiovascular causes. The finding of higher mortality in the intensive-therapy group led to a discontinuation of intensive therapy after a mean of 3.5 years of follow-up.

23
During follow-up, the primary outcome occurred in 352 patients in the intensive-therapy group, as compared with 371 in the standard-therapy group (hazard ratio, 0.90; 95% confidence interval [CI], 0.78 to 1.04; P=0.16). At the same time, 257 patients in the intensive-therapy group died, as compared with 203 patients in the standard-therapy group (hazard ratio, 1.22; 95% CI, 1.01 to 1.46; P=0.04). Hypoglycemia requiring assistance and weight gain of more than 10 kg were more frequent in the intensive-therapy group (P<0.001).
![During follow-up, the primary outcome occurred in 352 patients in the intensive-therapy group, as compared with 371 in the standard-therapy group (hazard ratio, 0.90; 95% confidence interval [CI], 0.78 to 1.04; P=0.16).](http://images.slideplayer.pl/38/10828459/slides/slide_23.jpg "At the same time, 257 patients in the intensive-therapy group died, as compared with 203 patients in the standard-therapy group (hazard ratio, 1.22; 95% CI, 1.01 to 1.46; P=0.04). Hypoglycemia requiring assistance and weight gain of more than 10 kg were more frequent in the intensive-therapy group (P<0.001)..")
24
General atherosclerosis Harm of hypoperfusion

25
The effect of RAAS blockade on the progression of diabetic nephropathy Sara S. Roscioni, Hiddo J. Lambers Heerspink and Dick de Zeeuw Nat. Rev. Nephrol. 10, 77–87 (2014)
.")
26
Roscioni, S. S. et al. Nat. Rev. Nephrol. 10, 77–87 (2014))
)")
27
Roscioni, S. S. et al. Nat. Rev. Nephrol. 10, 77–87 (2014).
.")
28
Roscioni, S. S. et al. Nat. Rev. Nephrol. 10, 77–87 (2014)
")
29
The gut–renal axis: do incretin-based agents confer renoprotection in diabetes? Marcel H. A. Muskiet, Mark M. Smits, Linde M. Morsink and Michaela Diamant Nat. Rev. Nephrol. 10, 88–103 (2014)
.")
30
Muskiet, M. H. A. et al. Nat. Rev. Nephrol. 10, 88–103 (2014); The gut–renal axis
; The gut–renal axis")
31
Muskiet, M. H. A. et al. Nat. Rev. Nephrol. 10, 88–103 (2014);
;")
32
Nie ma jednolitego patomechanizmu cukrzycowego uszkodzenia nerek, obejmującego wszystkich chorych Są różnice między cukrzycą typu 1 i 2 Przyspieszony proces miażdżycowy bywa głównym wyznacznikiem ubytku filtracji, zwłaszcza u starszych osób Podsumowanie

Podobne prezentacje